Chapter: Medicine Study Notes : Paediatrics
Causes of Developmental Delay
Causes of Developmental Delay
·
Causes of abnormal development:
o Environmental
o Genetic (eg chromosomal, metabolic)
o Disability (vision, hearing, motor)
o Brain injury (hypoxia, trauma, toxins, infection, prenatal &
post-natal)
o Illness, nutrition
o Unknown
Hearing
·
1 in 500 has significant
permanent hearing loss ® receptive and/or expressive language delay
·
All infants babble, even hearing
impaired
·
Suspect deafness when:
o Parental concern
o At risk babies (should be routinely screened):
§ Family history
§ Inter-uterine infection: rubella, CMV
§ Defects of ENT: cleft palate, external ear
§ Low birth weight
§ Neonatal distress
o Poor response to sound
o Not using words by 15 months
o General developmental delay
o Poor speech, comprehension and hearing failure
o Following brain trauma, infection, neurotoxic drugs
o Recurrent or persistent ear infections
· Normal development: See Topic: Development Chart: normal development from 0-60 months
·
History:
o Can he hear – how do you know?
o Previous development: first word, use of consonants, etc. Check Well Child Book
o Ear infections
o Antenatal: rubella, prematurity, jaundice, drugs
o Family history of hearing problems, developmental delay, neuro problems
· Exam:
o Dysmorphic features: cleft palate, external ear, skin, heart murmurs,
liver enlargement, normal genitalia
o Basic neuro exam, gait, symmetry of movement (including face), eye
movement
·
Investigations:
o Tympanogram
o Don‟t do distraction testing – hard unless you‟re well trained. Send straight for audiology
o Others depending on clinical findings: eg if regression then EEG, brain
scan, check stressors, chromosome problems, CK for Duchenne‟s
·
Differential of language delay:
o End of normal range
o Deafness
o Isolated language delay (usually expressive more delayed than receptive – but not necessarily)
o General delay or mild intellectual handicap ® formal
cognitive testing
o Autism
o Epilepsy: absence seizures – especially if fluctuates or regressive
o Possibly poor environment with little stimulation – but would also
expect ¯socialisation and ¯self care
o Congenital problems: cleft palate, macroglossia (eg Down‟s)
o Rare isolated CNS or motor problems
· Management: Speech language therapist, early intervention service, multidisciplinary team if problems over other domains. GP to support and co-ordinate, anticipate problems – especially at transitions (eg school, moving) and checking for comorbidity (eg behavioural problems, ¯self esteem)
·
Prognosis: Good if early
intervention – but maybe problems with higher language function (eg essay
writing)
Down Syndrome
· Trisomy 21: 47XY + 21
o Accounts for 95% of presentations of Down Syndrome. Usually (80%)
non-disjunction at first meiotic division
o 5% have different karyotypes:
§ Mosaic Down: 3 %
§ Robertsonian translocation t14:21: 4.8%
·
Epidemiology:
o Overall incidence is 1 in 700
o At least 20% still born
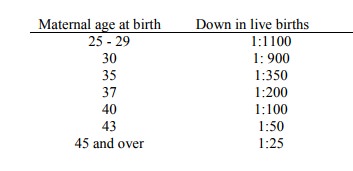
o Incidence increases with maternal age: at 16/40 gestation,
1 in 300 at 35 years, 1 in 22 at 45 years
o Accounts for 25% of children with IQ < 50
o ¼ of all chromosomal abnormalities. Chromosomal anomalies represent 15%
of congenital anomalies
o Risk:
· Neonatal Screening:
o Only 30% of children with Down are born to women over 35. Widespread screening of those > 35 will have only minor increase in detection rate
o Screening with the triple test will increase detection, but at the expense of significantly higher rates of invasive testing as there is a high false positive given the low incidence in younger women
·
Neonatal signs:
o Hypotonia
o ¯Moro
reflex
o Joint hyper-extensibility
o Excess skin at the back of the neck
o Flat facial profile
o Misshapen low set ears
o Protruding tongue
o Blunt inner eye angle
o Single palmer crease in 50%
o Clinodactyly (incurving) of little fingers in 50%
o Big „saddle‟ gap between big and 2nd toe
·
Complications:
o IQ generally from 45 – 55
o Congenital heart malformations in ~50%: VSD, ASD, patent ductus
o Susceptible to respiratory infections
o Duodenal atresia
o Also cataracts (2%), epilepsy (10%), hypothyroidism (3%), acute leukaemia (1%)
·
Development:
o Most will walk and develop simple language
o Puberty is often delayed and incomplete
o Average adult height is 150 cm
o Pre-senile dementia (similar to Alzheimer‟s disease) supervenes after
age 40
o 8% live past 40 years
Autism
· Onset before age 3 of:
o ¯Ability to form social relationships: slow to smile, don‟t enjoy being cuddled, indifferent eye contact
o ¯Use of both verbal and non-verbal communication: slow onset, echolalia, no use of gesture, poor pragmatics (eg turn taking and eye contact in conversation). If it was isolated language delay you would expect compensation in other areas (eg social) but here that‟s affected as well
o Restrictive and repetitive behavioural repertoire – dislike change
·
May start from birth, or regress
after normal development
·
Other behavioural problems:
outbursts, sleep problems, distractibility, poor toileting
·
Rare: 2 – 4/10,000. Boys = 3 *
girls
·
75% show some degree of general
intellectual impairment
·
Asperger‟s Syndrome:
o Symptoms overlap with autism
o Social interaction and behavioural problems similar to autism but not
associated with significant language or intellectual delay
Related Topics