Chapter: Medicine Study Notes : Paediatrics
Behavioural Issues - Paediatrics
Behavioural Issues
·
Behaviour doesn‟t exist outside
an environmental context
Behaviour Management
·
History Taking:
o Antecedent: what sets him off?
o Behaviour: describe exactly what he does?
o Consequence: What do you do about this?
· Principles:
o Remove (time out). Somewhere safe and boring, and where you don‟t mind the child disliking (ie not the toilet if toilet training or bedroom if sleep training). Leave a minute for every year of age.
o Be specific about what they‟re going in for. At the end, remind of the behaviour you want, and then forget the incident.
o Anticipate/avoid situations where conflict is likely
o Ignore minor things, particularly tantrums
o Distract
o Example (set a good one)
o Reward acceptable/wanted behaviour
·
Reward Systems:
o Star chart if young, more sophisticated and discrete if older
o Agreed between parents and child. Child
has to own it (can they help make it?)
o Planned: don‟t have to make a decision when the time comes
o Anticipated: known about in advance – When you this, then you will have …
o Consistently applied: no matter where he is or who he is with
o Immediate: not at the end of the week or when dad gets home from work
o Strong reward component
o Meaningful to child:
§ Young child: cuddles, praise and attention
§ 8+ years: if you … you can choose what we have for desert/which video,
etc (choice is powerful)
§ 10+: money
· Referral options:
o Special Education Service (SES): Resource teacher for learning and behaviour (RTLB) or Behaviour Support Team through SES
o Child psychiatry service (CAFS) if severe psychiatric symptoms (anxiety, depression, OCD, PTSD, sexually abused, ADD), persistent family dysfunction or resistant to simple management strategies
o Paediatrician if medical issues
o CYFS if abuse
·
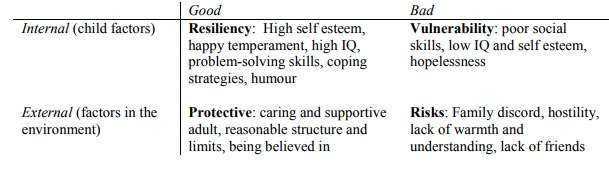
Attribution theory: Are their
successes and failures due to an internal locus of control („I passed the test
cause I did the work‟ ® high self-esteem) or an external locus of control („It doesn‟t matter
if I study or not, it won‟t make any difference‟ ® low self
esteem)
·
Individual traits the build
resiliency:
o Insight: recognition of ones‟ distressed condition with subsequent
action to overcome barriers
o Independence: gaining emotional distance and autonomy amid chaos
o Initiative: achievements that foster self confidence and constructive
activity
o Relationship building: Protective and nurturing connections with at least
one supportive adult
o Creativity: facilities healing and positive activity in a difficult
environment
o Humour: focuses on hope not harsh realities
o Morality: commitment to fairness and compassion
·
Family traits that build
resiliency:
o Commitment: loyalty, determination to work things out, sacrifice for
mutual benefit
o Cohesion: togetherness, respect for the individual, interdependence
o Adaptability: flexible, stress coping skills
o Communication: listening and speaking skills
o Spirituality: shared purpose and values
o Connectedness: Support within and beyond family, attitude of service
o Effective resource management: Competent use of money, time, etc
o Coherence: Optimism and self reliance
·
Intervention strategies:
o Provide opportunity for and encourage contributions
o Enhance decision making skills ® feeling of control
o Encourage and give positive feedback
o Develop self discipline: involve child in setting the rules and
consequences
Toddler Behaviour
·
Approach:
o History, including:
§ Antecedents, behaviours and consequences
§ Social context
§ Collaborative history if necessary
§ Psychiatric history from mother (is the child the problem?)
§ PMH: ABFWIMPS
o Exam: especially developmental
o Education
·
Most difficult behaviour does not
indicate a serious disturbance. Indicators of serious disturbance include:
o Deliberate self harm or messing
o Wandering off
o Running away
o Age inappropriate sexual behaviour
·
Developmental sequence of
everyday habits:
o Feeding
o Sleeping
o Eating
o Toilet
o Going to bed and getting up
o Dressing and undressing
o Washing and cleaning teeth
· Aim is to achieve regular habits and routines:
o To start with need to insist on regular routine and time schedule. Once achieved can be more flexible
o Failure to achieve routine: daily hassle and distress
o Regular routines ® security of child, ¯argument with parents
·
Factors which ¯behaviour
problems:
o Routine and regularity
o Clear limit setting
o Unconditional love and affection
o High level of supervision
o Consistent care and protection
o Age appropriate disciplines and rewards
·
Tantrums:
o Want their way. Purpose of tantrum is to get their way. Giving in reinforces the behaviour
o Must be consistent. If you say
no, will have to stick with it Þ choose your battles
o Options for managing a tantrum
§ Ignore it: eg leave the room
§ Time out
§ Distract
§ Avoid problem areas (eg supermarkets)
o Things will get worse before they get better. Once they realise the
boundaries are consistent they will stop testing them
·
Sleep Management:
·
Principles:
o Sleep is a learned process – you train your baby to do it
o After 6 months a night feed becomes a reward for waking up ® trained
night waker
o Parents also need time for themselves
·
For babies:
o Night feeds: quick, quiet, dim light
o Leave the baby to cry for a while
o Wrap them well, then not woken by their own reflexes (eg startle reflex
when lightly asleep)
·
Toddlers:
·
Evening routine: won‟t harm
toddler if you‟re firm with bedtime routines. No energetic games beforehand
·
Principles:
o Sleep is a learned process – you train your baby to do it
o After 6 months a night feed becomes a reward for waking up ® trained
night waker
o Parents also need time for themselves
·
For babies:
o Night feeds: quick, quiet, dim light
o Leave the baby to cry for a while
o Wrap them well, then not woken by their own reflexes (eg startle reflex
when lightly asleep)
·
Toddlers:
·
Evening routine: won‟t harm
toddler if you‟re firm with bedtime routines. No energetic games beforehand
·
Other points:
o Check parent‟s are not expecting too much of the child (eg 3 year old
boy not wetting at night)
o Keep no for important things
o All parents make mistakes
Problems at School
· ADHD
·
Symptoms:
o Normal IQ, no disabilities, but fail to develop academic potential
o Difficulty with peer relationships, loners, act out, difficult behaviour
o Develop associated problems: psycho-somatic, ¯self-esteem
·
Usually multifactorial:
o Constitutional factors: May have subtle defects in:
§ Receptive or expressive language
§ Auditory sequencing: can‟t remember verbal sequence (eg instructions). Can have a pervasive effect on schooling
§ Visual sequencing: difficulty reading/spelling
§ Motor problems (eg clumsy)
§ ¯Attention
(may be secondary to the above)
§ Health, hearing, vision, etc
o Environment: cultural, socio-economic status, family disruption, nutrition,
etc
o School related factors:
§ School factors associated with antisocial behaviour: poor morale, high turnover, inconsistent standards, undervaluing children‟s work, bullying
§ Kids spend 15,000 hours at school – so can have a big impact (just as family
does)
·
Assessment:
o History: parents
o Information from teachers
o Physical and neuro exam
o Sensory exam: vision and hearing
o Neuro-developmental, educational and psychological assessment
·
Management of Truancy:
o Educational programme appropriate for the child‟s needs
o Monitoring child through the day
o Assist with the learning process
Child in Trouble with the Authorities
·
History:
o Interview child and caregiver separately
o Presenting complaint
o History of presenting complaint:
§ Describe behaviour: Antecedents, Behaviours, Consequences
§ Social Context in which behaviour occurs: Relationships within family,
school, and peers. Physical or sexual abuse
§ Collaborative history: parents, teachers, sports coaches – this is
important
§ Psychiatric history: look for depression, anxiety, attentional problems
§ Formal assessment of learning if academic problems
·
Exam: especially dysmorphisms,
stature, neurocutaneous lesions, observations of reading, writing and
relationship with parents, vision and hearing
·
Development of antisocial behaviour:
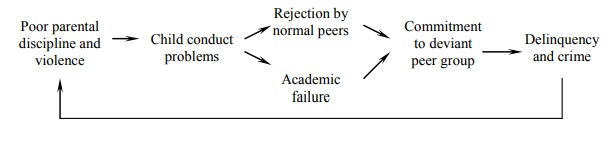
·
Possible differentials:
o Attachment disorder
o Developmental delay
o Behaviour conduct disorder
o Psychiatric illness: Depression, ADHD, PTSD (may appear to be
daydreaming)
o School refusal/Truancy
o Neglect or other abuse
o Domestic violence
·
Management plan:
o Keep in him school if at all possible: prognosis plummets if expelled or
regularly truant
o Ensure a thorough developmental assessment
o Referral for psych assessment and counselling
o Management: accentuate the positive, minimise the negative
o Referral to other services
Attachment Disorder
·
Attachment:
o Starts in utero and is an ongoing process
o Securely attached infants:
§ Are able to seek and obtain comfort from familiar caretakers
§ Are willing to explore and master their environment
o Insecurely attached infants (eg due to long separation from parents and
multiple carer-givers in hospital) appear:
§ Anxious: clingy without obvious stress
§ Avoidant: angry, distrustful of parents, won‟t be comforted after brief
separations
§ Indiscriminately affectionate: won‟t show preference for parents
·
Concepts:
o Separation: the process by which a child develops an identity separate from their parents.
o Promoted by secure attachment. At risk when the parents perceive the child is „vulnerable‟
o Autonomy: Development of independence (® social
competence)
o Mastery: increasing sense of competence over the physical environment
o Together autonomy and mastery lead to an internal locus of control.
Struggles for autonomy and mastery produce normal tantrums
· Types of Attachment Disorder:
o Disinhibited type: will go to anyone. No stranger awareness and constant, insatiable need for attention. Likely to be due to neglect. Also see it in chronic hospitalisation
o Withdrawn: frozen watchfulness, fearful. Likely to be due to abuse
·
Test by observing child when
parent leaves (separation), when a stranger comes in, and when parent returns
(reunion)
Domestic Violence
· Has significant health consequences: injury, psychiatric, chronic pain, drug and alcohol abuse
· Is common (some studies report up to 20% of women being hit in the last year), but often missed by doctors
·
Domestic violence starts with a
cycle of increasing control and disempowerment. Violence is used to reinforce
this
· Screening questions:
o „I have seen many people who come to see me with problems like yours. In my experience, many of these women are being hurt in some way by their partner. Is that happening to you?‟
o „A lot of tension and violence can be due to relationships within the
family – often with a partner. Is your partner being violent toward you?‟
·
Management:
o Ensure mum and the children are safe.
If not, refer to police/CYFS
o Refer to Women‟s refuge – be aware of the local services available
o Educate: eg the cycle or violence, it won‟t stop without help
o Avoid victim blaming („it‟s not your fault‟)
o Take careful notes (explain to the women why you are going this)
o Display information in your waiting room – signals a willingness to
discuss it
When Parents Separate
·
Responses to parent‟s separation
– all signs of distress:
o Withdrawn
o Clingy
o Regression
o Difficult behaviour
·
Helping the child:
o Accept the separation – then the child will too
o Make sure the child knows you love them
o Avoid conflict in front of the child
o Allow them to express their feelings
o Rely on other adults not the child for support
o Tell the kids they‟re not to blame
·
Things to avoid:
o Don‟t abuse their loyalty and trust
o Don‟t use them as messengers
o Don‟t use them to spy on other parent
o Don‟t continue to be angry at partner in front of them
o Don‟t let outings/gifts take the place of normal parenting
o Don‟t force kids to take sides
o Don‟t force a clash of loyalties
Related Topics