Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Hematologic Disorders
Disseminated Intravascular Coagulation (DIC)
DISSEMINATED
INTRAVASCULAR COAGULATION (DIC)
DIC is
not a disease but a sign of an underlying condition. DIC may be triggered by
sepsis, trauma, cancer, shock, abruptio pla-centae, toxins, or allergic
reactions (Chart 33-14). It is potentially life-threatening.
Pathophysiology
In
DIC, the normal hemostatic mechanisms are altered so that a massive amount of
tiny clots forms in the microcirculation. Ini-tially, the coagulation time is
normal. However, as the platelets and clotting factors are consumed to form the
microthrombi, coagulation fails. Thus, the paradoxical result of excessive
clotting is bleeding. The clinical manifestations of DIC are reflected in the
organs, which are affected either by excessive clot formation (with resultant
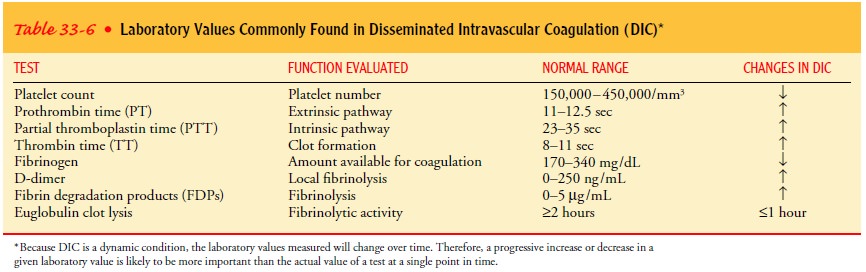
ischemia to all or part of the organ) or by bleeding. The bleeding is
characterized by low platelet and fibrinogen levels; prolonged PT, PTT, and
thrombin time; and elevated fibrin degradation products (D-dimers) (Table 33-6).
The
mortality rate can exceed 80% of patients who develop DIC. Identification of
patients who are at risk for DIC and recog-nition of the early clinical
manifestations of this syndrome can result in earlier medical intervention,
which may improve the prognosis. However, the primary prognostic factor is the
ability to treat the underlying condition that precipitated DIC.
Clinical Manifestations
Patients
with DIC may bleed from mucous membranes, venipunc-ture sites, and the
gastrointestinal and urinary tracts. The bleeding can range from minimal occult
internal bleeding to profuse hemorrhage from all orifices. Patients may also
develop organ dysfunc-tion, such as renal failure and pulmonary and multifocal
central nervous system infarctions as a result of microthromboses,
macro-thromboses, or hemorrhages.
During
the initial process of DIC, the patient may have no new symptoms, the only
manifestation being a progressive decrease in the platelet count. As the
thrombosis becomes more extensive, the patient exhibits signs and symptoms of
thrombosis in the organs involved. Then, as the clotting factors and platelets
are consumed to form these thrombi, bleeding occurs. Initially the bleeding is
subtle, but it can develop into frank hemorrhage. Signs and symp-toms depend on
the organs involved and are listed in Table 33-7.
Medical Management
The
most important management issue is treating the underlying cause of the DIC.
Until the cause is controlled, the mechanism for DIC will persist. A second
goal is to correct the secondary effects of tissue ischemia by improving
oxygenation, replacing fluids, cor-recting electrolyte imbalances, and
administering vasopressor med-ications. If serious hemorrhage occurs, the
depleted coagulation factors and platelets may be replaced to reestablish the
potential for normal hemostasis and thereby diminish bleeding. Cryoprecipitate
is given to replace fibrinogen and factors V and VII; fresh frozen plasma is
administered to replace other coagulation factors.
A
controversial method to interrupt the thrombosis process is the use of heparin
infusion. Heparin may inhibit the formation of microthrombi and thus permit
perfusion of the organs (skin, kidneys, or brain) to resume. Heparin is
typically reserved for the patient in whom thrombotic manifestations
predominate or in whom extensive blood component replacement fails to halt the
hemorrhage or increase fibrinogen and other clotting levels. When heparin is
administered, bleeding may actually worsen initially until the thrombotic
process is interrupted. Consumed platelets and clotting factors need to be
replaced. The effectiveness of heparin can best be determined by observing for
normalization of the plasma fibrinogen concentration and diminishing signs of
bleeding.
Related Topics