Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Hematologic Disorders
Bleeding Disorders
Bleeding Disorders
Normal
hemostatic mechanisms can control bleeding from ves-sels and prevent
spontaneous bleeding. The bleeding vessel con-stricts and platelets aggregate
at the site, forming an unstable hemostatic plug. Circulating coagulation
factors are activated on the surface of these aggregated platelets, forming
fibrin, which anchors the platelet plug to the site of injury.
The
failure of normal hemostatic mechanisms can result in bleeding, which is severe
at times. This bleeding is commonly provoked by trauma, but in certain
circumstances it can occur spontaneously. When the source is platelet or
coagulation factor abnormalities, the site of spontaneous bleeding can be
anywhere in the body. When the defect is caused by vascular abnormalities, the
site of bleeding may be more localized. Some patients have defects in more than
one hemostatic mechanism simultaneously.
In a
variety of situations, the bone marrow may be stimulated to increase platelet
production (thrombopoiesis). The increased production may be a reactive
response, as in a compensatory re-sponse to significant bleeding, or a more
general response to in-crease hematopoiesis, as in iron deficiency anemia.
Sometimes, the increase in platelets does not result from increased production
but from a loss in platelet pooling within the spleen. The spleen typically
holds about one third of the circulating platelets at any time. If the spleen
is lost (eg, splenectomy), the platelet reservoir is also lost, and an
abnormally high amount of platelets enter the circulation. In time, the rate of
thrombopoiesis slows to reestab-lish a more normal platelet level.
Clinical Manifestations
Signs
and symptoms of bleeding disorders vary depending on the type of defect. A
careful history and physical examination can be very useful in determining the
source of the hemostatic defect. Ab-normalities of the vascular system give
rise to local bleeding, usu-ally into the skin. Because platelets are primarily
responsible for stopping bleeding from small vessels, patients with platelet
defects develop petechiae, often in clusters; these are seen on the skin and
mucous membranes but also occur throughout the body. Bleed-ing from platelet
disorders can be severe. Unless the platelet dis-order is severe, bleeding can
often be stopped promptly when local pressure is applied; it does not typically
recur when the pressure is released.
In
contrast, coagulation factor defects do not tend to cause su-perficial
bleeding, because the primary hemostatic mechanisms are still intact. Instead,
bleeding occurs deeper within the body (eg, subcutaneous or intramuscular
hematomas, hemorrhage into joint spaces). External bleeding diminishes very
slowly when local pressure is applied; it often recurs several hours after
pressure is removed. For example, severe bleeding may start several hours after
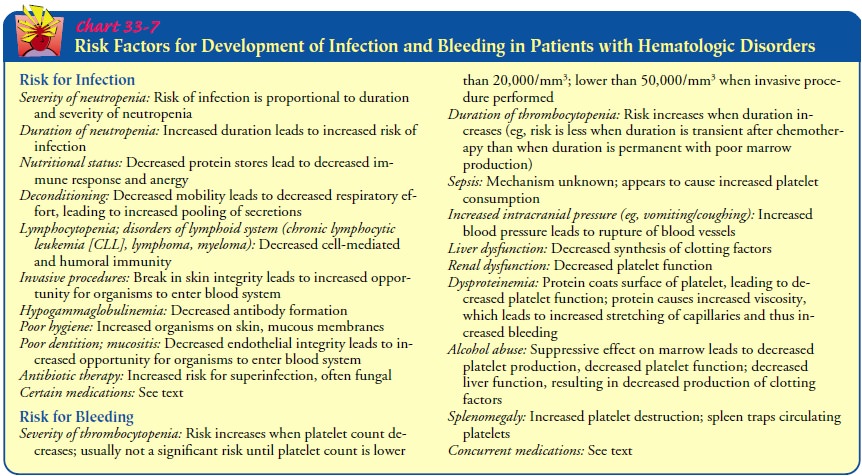
a tooth extraction. Risk factors for bleeding are provided in Chart 33-7.
Medical Management
Management
varies based on the underlying cause of the bleed-ing disorder. If bleeding is
significant, transfusions of blood prod-ucts are indicated. The specific blood
product used is determined by the underlying defect. In specific situations in
which fibrino-lysis is excessive, hemostatic agents such as aminocaproic acid
(Amicar) can be used to inhibit this process. This agent must be used with
caution, because excessive inhibition of fibrinolysis can result in thrombosis.
Nursing Management
Patients
who have bleeding disorders or who have the potential for development of such
disorders as a result of disease or thera-peutic agents must be taught to
observe themselves carefully and frequently for bleeding. They need to
understand the importance of avoiding activities that increase the risk of
bleeding, such as contact sports. The skin is observed for petechiae and
ecchymoses (bruises) and the nose and gums for bleeding. Hospitalized pa-tients
may be monitored for bleeding by testing all drainage and excreta (feces,
urine, emesis, and gastric drainage) for occult as well as obvious blood.
Outpatients are often given fecal occult blood screening cards to detect occult
blood in stools.
Related Topics