Chapter: The Massage Connection ANATOMY AND PHYSIOLOGY : Skeletal System and Joints
TemporoMandibular Joint (TMJ)
TEMPOROMANDIBULAR JOINT (TMJ)
The temporomandibular joint (see Figure 3.35) is af-fected by dysfunction and disease in more than 20% of the population at sometime in their life. It is a complex joint; its function is affected by multiple structures such as the bones of the skull; mandible; maxilla; hyoid; clavicle; sternum; the joint between the teeth and the alveolar cavities; muscle and soft tissue of the head and neck; and muscles of the cheeks, lips, and tongue. It is affected by the posture of the head and neck and cervical curvature. The joint is used almost continuously for chewing, swal-lowing, respiration, and speech. Imbalance relating to any of the associated structures can affect this joint. Conversely, problems relating to the joint can reflect as dysfunction of any of the associated struc-tures. Hence, dysfunction of this joint is difficult to diagnose and manage.
Articulating Surfaces and Type of Joint
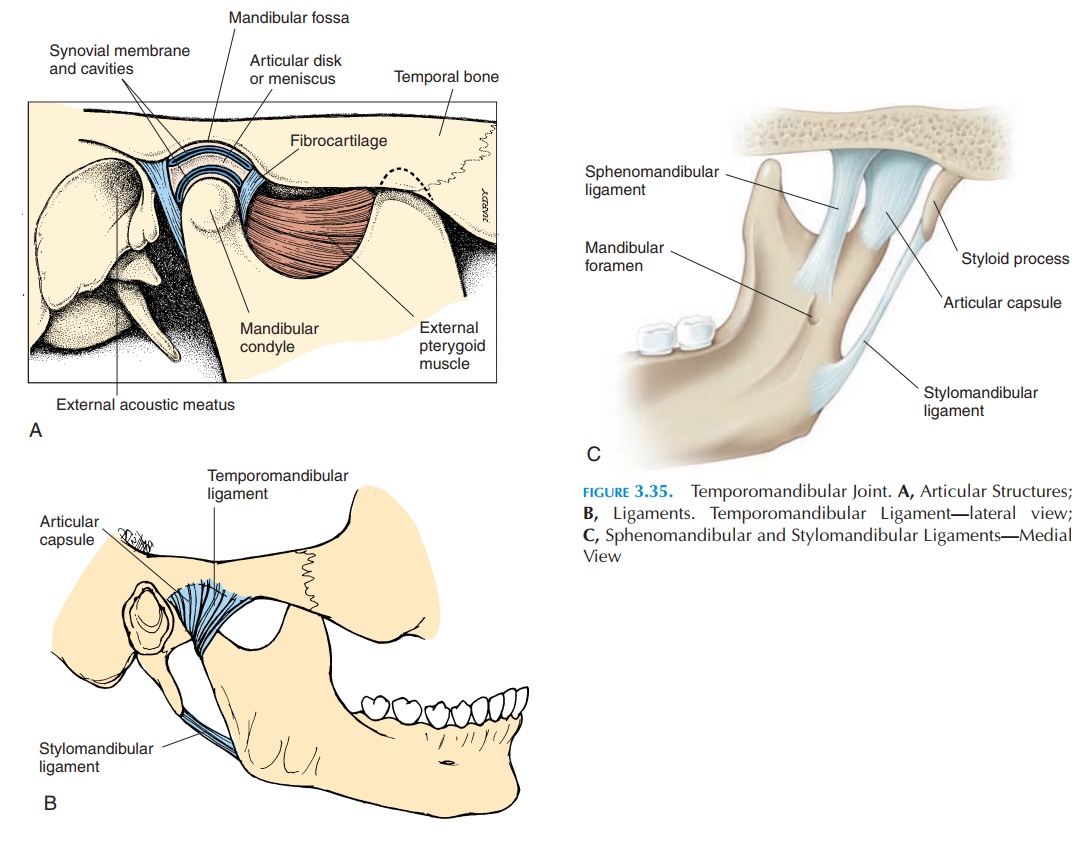
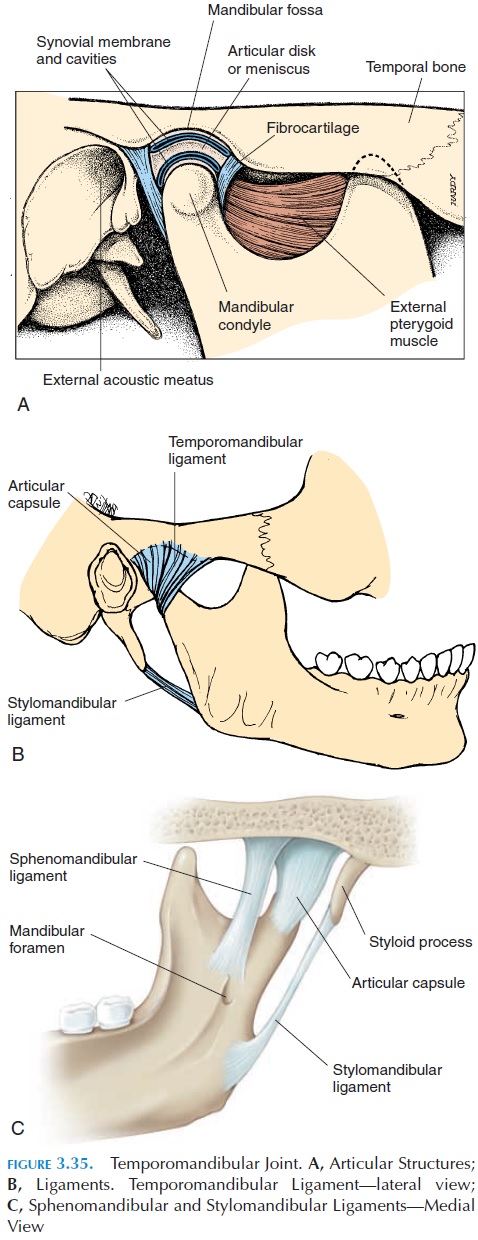
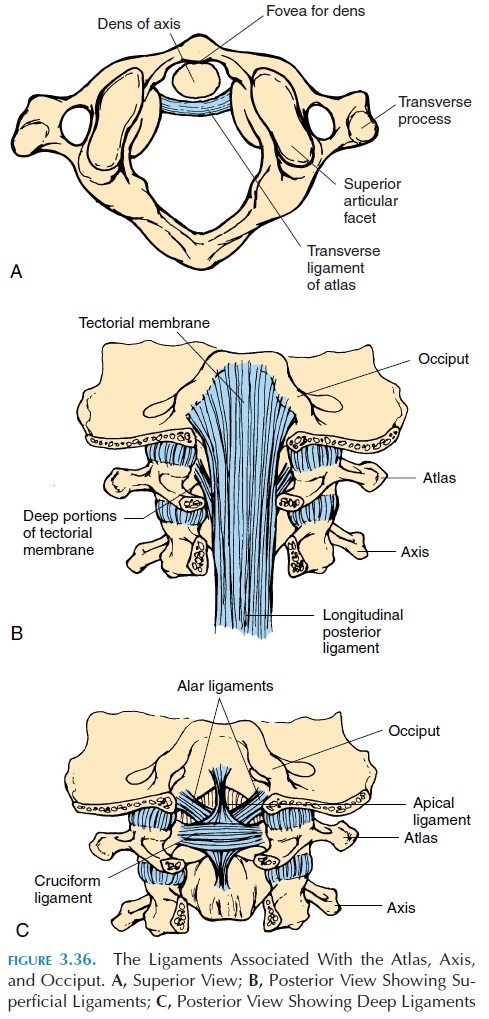
The mandibular condyle articulates with the mandibu-lar fossa of the temporal bone in this joint (see Figure 3.36). The surface of the fossa is concave posteriorly and convex anteriorly because of the articular emi-nence. The presence of an interarticular disk/carti-lage/meniscus, compensates for the difference in the shapes of the two articular surfaces (the condyle has a convex surface). The disk also divides the joint into a superior and inferior cavity and, because of it, the ar-ticular surfaces of the bones are not in direct contact with each other. The outer edges of the disk are con-nected to the capsule. The joint is strengthened by lig-aments (Figure 3.35B and C). This joint is a combina-tion of a plane and a hinge joint.
Ligaments
The articular capsule, or capsular ligament, is a sleeve of thin, loose fibrous connective tissue that surrounds the joint. The lateral ligament (temporo-mandibular ligament) is a thickening of the capsulelaterally, positioned in the lateral side of the capsule under the parotid glands. It stabilizes the joint later-ally and prevents extensive anterior, posterior, and lateral displacement of the mandibular condyle. The stylomandibular ligament, not directly related tothe joint, extends from the styloid process to the pos-terior border of the ramus of the mandible. It pre-vents the mandible from moving forward extensively as when opening the mouth wide. The spheno-mandibular ligament stabilizes the joint mediallyand helps suspend the mandible when the mouth is opened wide.
Possible Movements
Depression and elevation of the mandible (hinge joint) and protraction and retraction (gliding joint) are possible. The mandible can also be moved laterally as a result of the presence of the articular carti-lage. The movement of the mandible is a result of the action of both cervical and mandibular muscles.
Range of Motion
Normally, three fingers can be inserted into the mouth between the incisor teeth.
Muscles
Muscles that open (depress) the jaw:
Primary depressors
External (lateral) pterygoid muscle Anterior head of the digastric
Secondary depressors
Gravity
Muscles attached to the hyoid bone (suprahyoid muscles—digastric, stylohyoid, mylohyoid, genio-hyoid—and infrahyoid muscles—sternohyoid, thyrohyoid, omohyoid)
Muscles that close (elevate) the jaw:
Primary elevators
Masseter
Temporalis
Secondary elevators
Internal (medial) pterygoid
(Superior head of the lateral pterygoid stabilizes the disk and condylar head during elevation)
Muscles that retract the jaw: Posterior fibers of the temporalis Deep fibers of the masseter Digastric
Suprahyoids
Muscles that protract the jaw: Medial pterygoid
Superficial fibers of the masseter Lateral movement:
Lateral and medial pterygoid on one side and con-tralateral temporalis muscle assisted by digas-tric, geniohyoid, and mylohyoid
Physical Assessment
A complete history of problems relating to the joint, in-cluding when it started, how it occurred, and previous management is important. History of habitual protru-sion and muscular tension is important. Difficulty opening and closing the mouth, frequent headaches, and abnormal sounds from joints are some symptoms associated with the joint dysfunction.
The posture of the person should be examined. Typically, the shoulders are elevated, with the head forward, a stiff neck and back, and shallow, restricted breathing. The area around the joint should be in-spected carefully. The movement of the jaw must be noted to ensure continuous, symmetrical movements. The alignment of the teeth should also be examined.
The movements of the condyle of the mandible can be palpated by placing the finger inside the external auditory canal. Clicking sounds may be present if the articular disk is damaged or if there is swelling. The pterygoid muscles can be palpated through the inside of the mouth (disposable gloves should be worn for this procedure). The range of motion—both active and passive—should be checked together with palpation of all relevant muscles for tender points (Refer to books on musculoskeletal assessment for more details).
Related Topics