Chapter: Ophthalmology: Cornea
Viral Keratitis
Viral Keratitis
Viral keratitis is frequently caused by:
❖ Herpes simplex virus.
❖ Varicella-zoster virus.
❖ Adenovirus.
Other rare
causes include cytomegalovirus, measles virus, or rubella virus.
Herpes Simplex Keratitis
Epidemiology and pathogenesis: Herpes simplex keratitis is among themore common causes of
corneal ulcer. About 90% of the population are car-riers of the herpes simplex
virus. A typical feature of the ubiquitous herpes simplex virus is an unnoticed
primary infection that often heals spon-taneously. Many people then remain
carriers of the neurotropic virus, which can lead to recurrent infection at any
time proceeding from the trigeminal ganglion. A corneal infection is always a recurrence. A primary herpes
simplex infection of the eye will present as blepharitis or conjunctivitis.
Recurrences may be triggered external influences (such as exposure to
ultraviolet light), stress, menstruation, generalized immunologic deficiency,
or febrile infec-tions.
Symptoms: Herpes simplex keratitis is usuallyvery painfuland associatedwith photophobia, lacrimation, and
swelling of the eyelids. Vision may be impaired depending on the location of
findings, for example in the presence of central epitheliitis.
Forms and diagnosis of herpes simplex keratitis: The following forms ofherpes simplex keratitis
are differentiated according to the specific layer of the cornea in which the
lesion is located. Recurrences are more frequent in the stroma and endothelium.
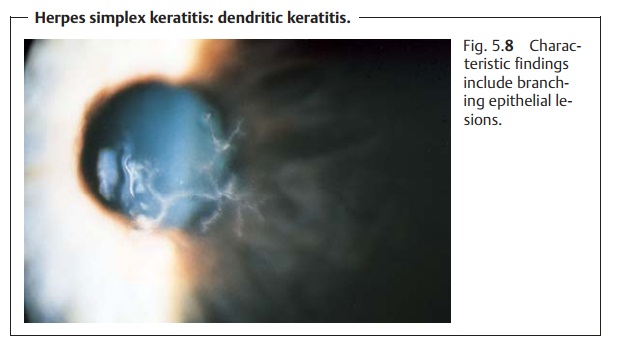
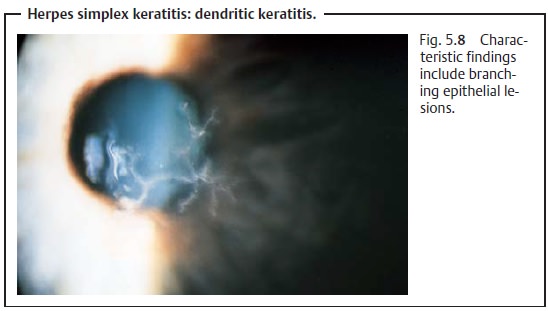
Dendritic keratitis.This is characterized by branching epithelial lesions(necrotic and vesicular swollen epithelial cells, Fig. 5.8). These findings will be visible with the unaided eye after application of fluorescein dye and are characteristic of dendritic keratitis. Corneal sensitivity is usually reduced.
Dendritic keratitis may progress to stromal
keratitis.
Stromal Keratitis.Purely stromal involvement without prior dendritic ker-atitis is
characterized by an intact epithelium that will not show any defects after
application of fluorescein dye. Slit lamp examination will reveal central diskiform corneal infiltrates (diskiform
keratitis) with or without a whitishstromal infiltrate. Depending on the
frequency of recurrence, superficial or deep vascularization may be present.
Reaction of the anterior chamber will usually be accompanied by endothelial
plaques (protein deposits on the pos-terior surface of the cornea that include
phagocytized giant cells).
Endotheliitis.Endotheliitis or endothelial keratitis is caused by the
presenceof herpes viruses in the aqueous humor. This causes swelling of the
endothelial cells and opacification of the adjacent corneal stroma.
Involve-ment of the endothelial cells in the angle of the anterior chamber
causes a secondary increase in intraocular pressure (secondary glaucoma). Other find-ings include inflamed cells and
pigment cells in the anterior chamber, and endothelial plaques; involvement of
the iris with segmental loss of pig-mented epithelium is detectable by slit
lamp examination.
Acute retinal necrosis syndrome.Involvement of the posterior eyeball (seeherpetic retinitis) for
all practical purposes is seen only in immunocom-promised patients (e.g.,
recipients of bone marrow transplants and AIDS patients).
Treatment: Infections involving theepitheliumare
treated with trifluridineas a superficial virostatic agent. Stromal and intraocular herpes simplex
infectionscan be treated with acyclovir, which is available for topical
use (inointment form) and systemic use.
Corticosteroids are contraindicated in
epithelial herpes simplex infec-tions but may be used to treat stromal
keratitis where the epithelium is intact.
Herpes Zoster Keratitis
Definition
Keratitis due to endogenous recurrence of
chickenpox (caused by the varicella-zoster virus; see herpes zoster
ophthalmicus).
Etiology: Proceeding from the trigeminal ganglion, the virus reinfects
theregion supplied by the trigeminal nerve. The eye is only affected where the
ophthalmic division of the trigeminal nerve is involved. In this case, the
naso-ciliary nerve supplying the interior of the eye will also be affected.
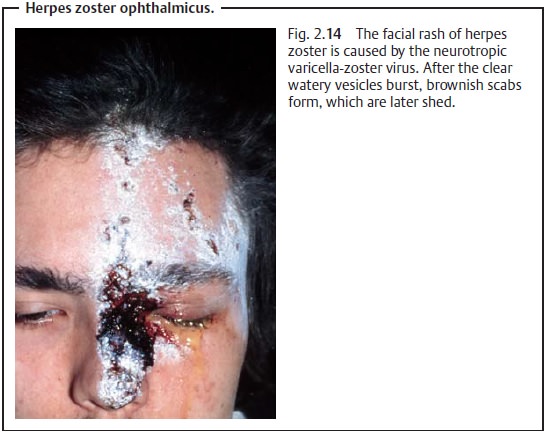
Hutchin-son’s sign, vesicular lesions on the tip of the nose, will be present
(see Fig. 2.14).
Diagnostic considerations: Herpes zoster ophthalmicus also occurs insuperficial and deep
forms, which in part are similar to herpes simplex infec-tion of the cornea
(red eye with dendritic keratitis, stromal keratitis, and ker-atouveitis).
Corneal sensitivity is usually decreased or absent.
Treatment: The eye is treated with acyclovir ointment in consultation with
adermatologist, who will usually treat skin changes with systemic acyclovir (in
the form of infusions or tablets). If the corneal epithelium is intact, the
irrita-tion of the anterior chamber can be carefully treated with steroids and
immo-bilization of the pupil and ciliary body by therapeutic mydriasis.
Related Topics