Chapter: Ophthalmology: Cornea
Cornea: Basic Knowledge
Cornea
Basic Knowledge
Fundamental importance of the cornea for the eye: The cornea is the eye’soptical window that
makes it possible for humans to see. The ophthalmolo-gist is only able to
discern structures in the interior of the eye because the cor-nea is
transparent. At 43 diopters, the cornea is the most important refractivemedium in the eye.
Shape and location: The cornea’scurvature is
greater than the sclera’s curva-ture. It fits into the sclera like a watch-glass with a shallow sulcus (the
limbusof the cornea) marking the junction of the two structures.
Embryology: The corneal tissue consists offive layers. The cornea and thesclera are formed during the second
month of embryonic development. The epithelium develops from ectoderm, and the
deeper corneal layers develop from mesenchyme.
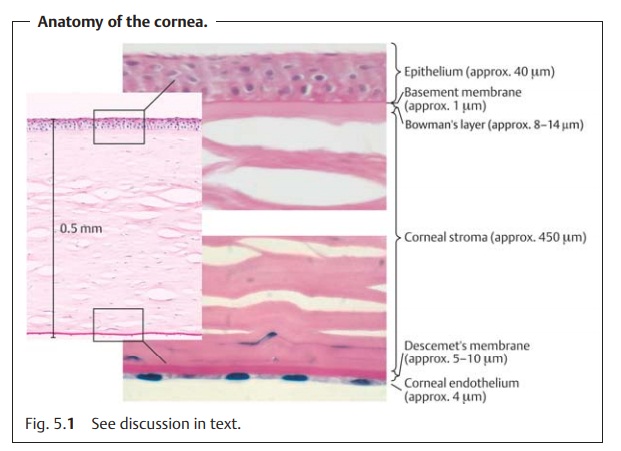
Morphology and healing (Fig. 5.1):
❖Thesurface of the cornea is formed by stratified
nonkeratinizedsquamous epithelium that regenerates quickly when injured. Within ahour, epithelial
defects are closed by cell migration and rapid cell division. However, this
assumes that the limbus stem cells in
the limbus of the cor-nea are undamaged. Regular corneal regeneration will no
longer be possible when these cells are compromised. An intact epithelium
protects against infection; a defect in the epithelium makes it easy for
pathogens to enter the eye.
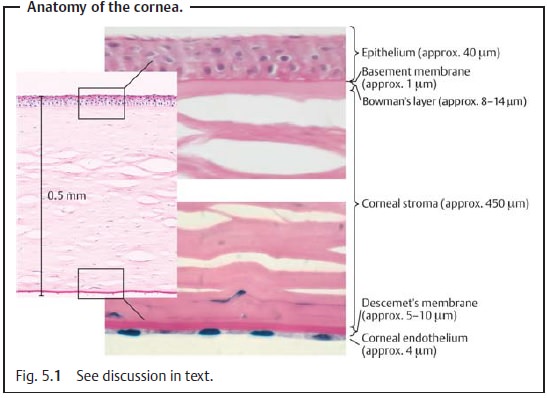
❖A thin basement membrane anchors the basal cells of the stratified squamous
epithelium to Bowman’s layer. This layer is highly resistant but cannot regenerate. As a
result, injuries to Bowman’s layer usually produce corneal scarring.
❖ Beneath Bowman’s layer, many lamellae of collagen fibrils form the cor-neal stroma. The stroma is a highly bradytrophic tissue. As avasculartissue, it only regenerates slowly. However, its avascularity makes it an immunologically privileged site for grafting. Routine corneal transplantsmay be performed without prior tissue typing. An increased risk of rejection need only be feared where the recipient’s cornea is highly vascularized as may be the case following chemical injury or inflammation. Such cases require either a tissue-typed donor graft or immunosuppressive therapy with cyclosporin.
❖ Descemet’s membrane and the corneal
endothelium lie on the posterior surface of the corneal stroma adjacent to the
anterior chamber. Descemet’s membrane is a relatively strong membrane. It will
continue todefine the shape of the anterior chamber even where the corneal
stroma has completely melted (see Descemetocele). Because it is a genuine base-ment membrane, lost tissue is
regenerated by functional endothelial cells.The corneal endothelium is responsible for the transparency of the cornea (see also Transparency below). A high
density of epithelial cells is neces-sary to achieve this. The corneal
endothelium does not regenerate; defects in the endothelium are closed by cell
enlargement and cell migration.
Diameter: Thenormal average
diameter of the adult corneais 11.5 mm(10 – 13 mm). A congenitally small
cornea (microcornea, diameter less
than 10.0 mm) or a congenitally large cornea (megalocornea, diameter from 13 to 15 mm) is always an abnormal
finding (see Corneal Size Anomalies).
Nourishment: The five layers of the cornea have few cells and are
unstruc-tured and avascular. Like the lens, sclera, and vitreous body, the
cornea is a bradytrophic tissue structure. Its metabolism is slow, which means
that heal-ing is slow. The cornea is nourished with nutritive metabolites
(amino acids and glucose) from three sources:
·
Diffusion from the capillaries at its edge.
·
Diffusion from the aqueous humor.
·
Diffusion from the tear film.
Significance of the tear film for the cornea: The three-layer precorneal tearfilm ensures
that the surface of the cornea remains smooth and helps to nour-ish the cornea
(see above). Without a tear film, the surface of the epithelium would be rough,
and the patient would see a blurred image. The enzyme lysozyme contained in the
tear film also protects the eye against infection (for composition of the tear
film).
Transparency: This is due to two factors.
The uniform arrangement of the lamellae of collagen fibrils in the cor-neal stroma and the smooth endothelial and epithelial surface producedby the intraocular pressure.
The water content of the corneal stroma remains
constant at 70%. The combined
action of the epithelium and endothelium maintains a constant water content;
the epithelium seals the stroma off from the outside, while the endothelium
acts as an ion pump to remove water from the stroma. This requires a sufficiently high density of endothelial
cells. Endothelial cell density is age-dependent; normally it is
approximately 2500 cells per mm2. At cell densities below 300 endothelial cells per mm2, the endothelium is no longer able to pump water out of the
cornea, resulting in edema of the corneal stroma and endothelium.
Protection and nerve supply: The cornea is a vital structure of the eye and asa result
extremely sensitive. It receives its ample
sensory supply from the oph-thalmic division of the trigeminal nerve. The
slightest tactile sensation causes an eye closing reflex. Any injury to the
cornea (erosion, foreign body penetra-tion, or ultraviolet
keratoconjunctivitis) exposes sensory nerve endings and causes intense pain
with reflexive tearing and involuntary eye closing.
The triad of involuntary eye closing
(blepharospasm), reflexive tearing (epiphora), and pain always suggests a
possible corneal injury.
Related Topics