Chapter: Ophthalmology: Cornea
Curative Corneal Procedures
Curative Corneal Procedures
Penetrating Keratoplasty (Fig. 5.18a)
Principle: This involves replacement of diseased corneal tissue with a
full-thickness donor graft of corneal tissue of varying diameter. A clear, regularly
refracting button of donor cornea is placed in an opacified or irregularly
refracting cornea. The corneal button is sutured with a continuous single or
double suture (Fig. 5.19) or with
interrupted sutures. (For special considera-tions in corneal transplants, see
also Morphology and healing.)


Penetrating keratoplasty can be performed as
an elective procedure to improve visual acuity or as an emergency procedure (emergency kerato-plasty). Emergency keratoplasty is indicated to treat a perforated or
nonheal-ing corneal ulcer to remove the perforation site and save the eye (tectonic ker-atoplasty).
Indications: Corneal diseases that affect the full thickness of the
cornealstroma (corneal scars, dystrophy, or degeneration) or protrusion
anomalies such as keratoconus or keratoglobus with or without central corneal
opacification.

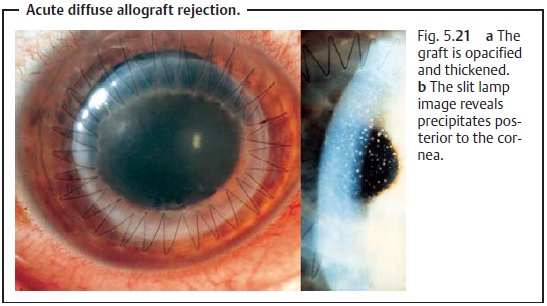
Allograft Rejection (Complications): The body’s immune system canrespond with a chronic focal allograft rejection (Fig. 5.20) or a diffuse allograft rejection (Fig. 5.21). The graft will be become opacified.
Lamellar Keratoplasty (Fig. 5.18b)
Principle: This involves replacement of a superficial stromal
opacificationwith a partial-thickness donor graft of clear corneal tissue.
This surgery requires the corneal epithelium, Descemet’s membrane, and the deeper layers of the cornea to be intact and healthy as it is only suitable for removing superficial opacifications down to about the middle of the cornea. The donor corneal button is then sutured with one or two continuous sutures or with interrupted sutures.
Indications: Corneal opacifications and scars affecting the superficial
cornealstroma (post-traumatic, degenerative, dystrophic, or postinflammatory
opacifications). This method is not suitable for treating corneal ulcers.
Allograft Rejection (Complications): Allograft rejection is less frequent thanin
the case of penetrating keratoplasty. There is also less danger of infection as
lamellar keratoplasty does not involve opening the globe.
Phototherapeutic Keratectomy (Fig. 5.18c)
Principle: Superficial corneal scars can be ablated with an excimer
laser(wavelength of 193 nm). The lesion is excised parallel to the surface of
the cor-nea to avoid refractive effects. The edges of the ablated area are
merged smoothly with the rest of the corneal surface, eliminating any
irregularities.
Indications: Indications are identical to those for lamellar
keratoplasty.However, this method is only suitable for ablation of relatively
superficial cor-neal opacifications, i.e., in the upper 20% of the corneal
stroma.
Disadvantage: Despite attempting ablation parallel to the surface of the
cor-nea, phototherapeutic keratectomy often creates a hyperopic effect.
Related Topics