Chapter: Ophthalmology: Cornea
Cornea: Developmental Anomalies
Developmental Anomalies
Protrusion Anomalies
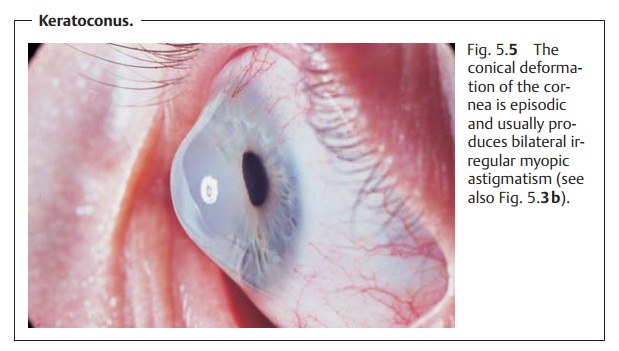
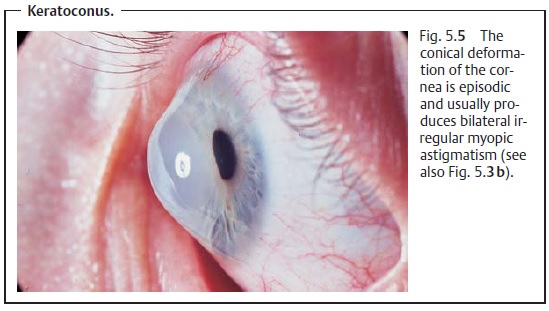
Keratoconus
Definition
Conical, usually bilateral central deformation
of the cornea with parenchymal opacification and thinning of the cornea.
Epidemiology: Keratoconus is the mostfrequently
encountereddeformationof the cornea. Occurrence is familial, although women
are more likely to be affected than men.
Etiology: Keratoconus is probably a genetic disorder. It can occur in familieswith varying paths of hereditary transmission. Occasionally keratoconus is associated with trisomy 21 syndrome (Down syndrome) as well as with atopic dermatitis and other connective-tissue disorders such as Marfan’s syn-drome.
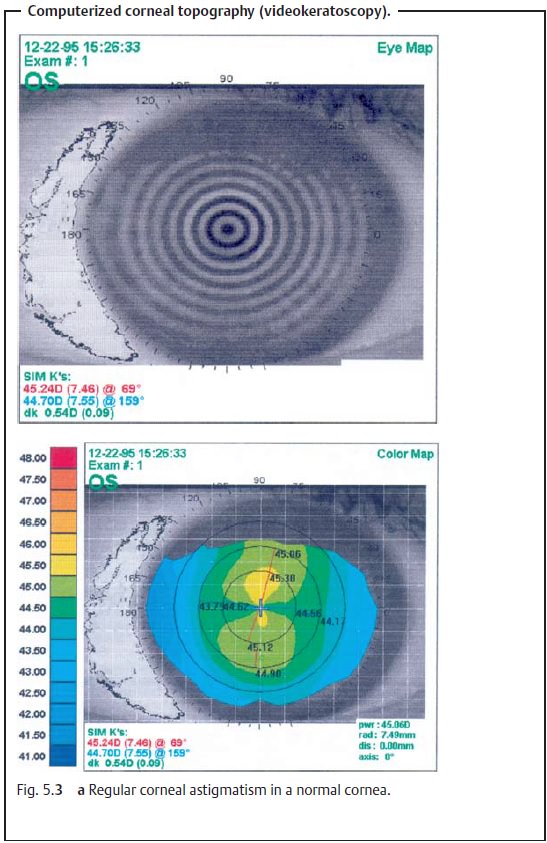
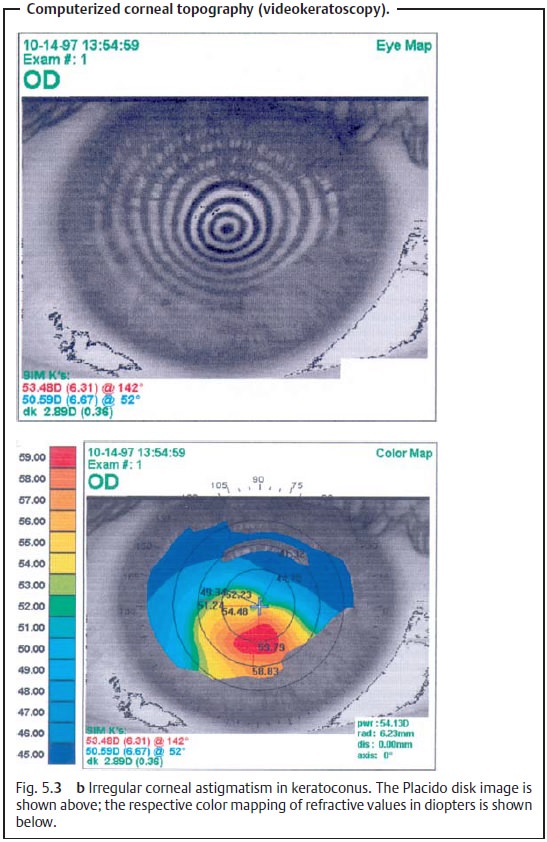
Symptoms: The clinical course of the disorder is episodic; the increasing
pro-trusion of the cornea usually produces bilateral irregular myopic
astigmatism (see Fig. 5.3b). Left
untreated, in rare cases keratoconus can cause tears of Descemet’s membrane due
to the continuous stretching. The entire cornea can then bulge out at this
site. This is referred to as acute keratoconus. Symp-toms of acute keratoconus include sudden loss of visual acuity
accompaniedby intense pain, photophobia, and increased tearing.
Diagnostic considerations: The diagnosis is usually made with a kerato-scope or
ophthalmometer (reflex images will be irregular). The examiner can also detect
keratoconus without diagnostic aids by standing behind the patient and pulling
the patient’s upper eyelids downward. The conical protru-sion of the surface of
the cornea (Fig. 5.5) will then be
readily apparent due to the deformation of the margin of the eyelid (Munson’s sign).
Treatment: Degeneration of visual acuity can usually be corrected
initiallywith eyeglasses; hard contact lenses will be required as the disorder
prog-resses. However, after a certain point, the patient repeatedly will lose
the con-tact lenses. Then the only possible treatment is penetrating
keratoplasty (transplantation of a corneal graft from a donor into the
patient’s cornea).
Prognosis: The prognosis for penetrating keratoplasty in treating kerato-conus is good because the cornea is avascular in keratoconus.
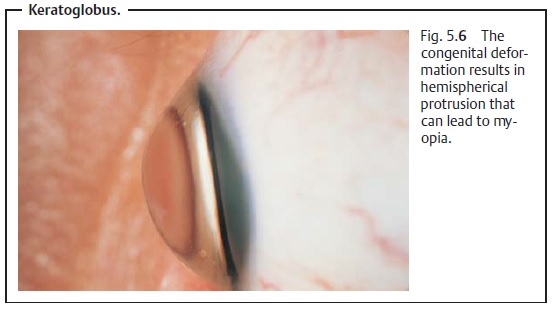
Keratoglobus
Very rare disorders include keratoglobus, a
congenital deformation resulting in hemispherical protrusion (Fig. 5.6) that tends to produce
myopia, and flat-tening of the cornea (cornea plana) that tends to produce
hyperopia.
Corneal Size Anomalies (Microcornea and Megalocornea)
Corneal size anomalies are usually congenital
and on the whole are rare. An abnormally small cornea (microcornea) has a diameter less than 10.0 mm). It usually causes severe
hyperopia that in advanced age often predisposes the patient to angle closure
glaucoma (see Table 10.2). An abnormally large cornea (megalocornea) may be as large as 13 – 15 mm. Corneal enlarge-ment in the
newborn and infants may be acquired due to increased intraocu-lar pressure
(buphthalmos). Combinations of microcornea and megalocor-nea together with other ocular deformities may
also occur.
Related Topics