Chapter: Case Study in Obstetrics and Gynaecology: General Obstetrics
Case Study Reports: Pain in Pregnancy
PAIN IN PREGNANCY
History
A
33-year-old Asian woman complains of worsening abdominal
pain for 4 days. She is
16 weeks pregnant in her
third pregnancy. She
has a 10-year-old son, by normal delivery, and had a miscarriage 8 years ago. Her pregnancy has been uneventful until now with an
unremarkable first-trimester scan.
The
pain is in the left lower abdomen
and is constant and sharp.
She has taken paracetamol
with little effect
and she is unable to sleep due to the pain.
She
has had no vaginal bleeding and reports urinary
frequency since the
beginning of the pregnancy. She is mildly
constipated and has no nausea
and vomiting. There
is no history of trauma. She has not felt the baby moving yet.
Examination
The
woman is apyrexial and pulse rate is 125/min,
with blood pressure
110/68 mmHg. The uterus is palpable just
above the umbilicus. There is significant tenderness over the left uterine fundal region,
where it also
feels firm. The
abdomen is otherwise soft and
non-tender. There is voluntary guarding
but no rebound tenderness. Bowel
sounds are normal.
Speculum examination shows a normal,
closed cervix and no blood.
The fetal heart-
beat is heard with hand-held fetal Doppler.
Questions
·
What is the likely diagnosis and how should it be confirmed?
·
How would you manage this woman?
·
What effect will this condition have on the pregnancy?
ANSWER
The
diagnosis is of fibroid degeneration. The uterine size
larger than dates
and the local- ized uterine tenderness are the important features in making
this diagnosis. Fibroids
affect 20–30 per cent
of the female
population, commonly developing between 30 and
50 years. They are particularly common
in African-Caribbean women.
Fibroids are oestrogen sensitive and therefore grow in pregnancy in response
to the hyperoe- strogenic state. When they outgrow their blood supply they undergo ‘red degeneration’, with
necrosis within the fibroid
causing the intense localized pain. The diagnosis of fibroids
is con- firmed by ultrasound visualization of an encapsulated mass in the uterus.
The degeneration is confirmed by the ultrasound
appearance of cystic spaces within the fibroid
mass.
Degeneration pain usually starts
gradually, and some women manage
at home with sim-
ple paracetamol and
rest until the
pain subsides. However, it is common
for the pain
to be severe enough
for admission to hospital for opiate analgesia. Opiates are safe in preg- nancy provided use is not prolonged. Intravenous fluids may be required
if the woman is not drinking, or is vomiting
due to the pain.
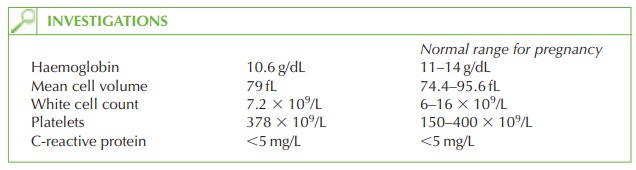
Most women remain well systemically, although
a full blood count and C-reactive protein should be taken to check haemoglobin and to assess
the white blood
count and inflamma- tory markers. In this case the woman has a mild microcytic anaemia
of pregnancy and should be given ferrous sulphate.
The
pregnancy itself is not usually
compromised by degenerating fibroids except in the
rare cases where sepsis develops, in which case miscarriage may occur.
Fibroids are managed expectantly in pregnancy but
may cause malpresentation at term, or obstructed labour if there
is a pelvic fibroid. In either of these circumstances, Caesarean section should be performed. Most fibroids shrink during the puerperium, so consideration
of surgery should be deferred
for at least 3 months after delivery.

Related Topics