Chapter: Case Study in Obstetrics and Gynaecology: General Obstetrics
Case Study Reports: Antenatal Screening
ANTENATAL SCREENING
History
A
woman aged 34 years is 9 weeks’
gestation in her third pregnancy. Her first pregnancy ended in a first-trimester suction termination at 18 years
of age and
she had a miscarriage
8 months ago requiring evacuation of retained products of conception (ERPC).
She is gen- erally well except for mild asthma.
She
has no family
history of congenital abnormalities. She is a non-smoker and currently
drinks approximately 3 units of alcohol per week. Her only medication is folic acid 400 μg daily.
Her partner is 31 years old and was
adopted. He has no known medical problems.
The
routine booking blood
and urine tests
are normal. The couple opt for Down’s
syndrome screening and a first-trimester ultrasound appointment is booked
for 12 weeks.
Questions
·
How
would you explain
the report to the couple?
·
What are the options
available to the
couple now and
what are their
relative advan- tages and disadvantages?
·
The
couple chose to have a further test
and the results
are normal, what
further diag- noses should
be considered?
ANSWER
Explanation of the report
Down’s syndrome screening can be difficult to explain, and any discussion should start with checking
that the couple
understand what Down’s
syndrome is:
·
a
chromosomal ‘genetic’ problem
that usually occurs
sporadically (‘by chance’)
·
associated with physical abnormalities which may be relatively minor,
such as short stature, abnormal facial appearance, or major, such
as severe cardiac
abnormality
·
always associated with learning
disability, though the extent is variable
·
life expectancy is generally
up to 40 or 50 years.
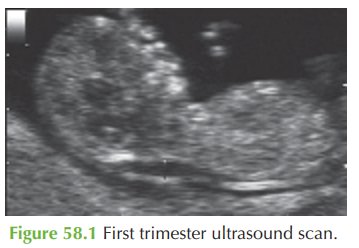
The
‘nuchal translucency’ test
is a screening test and
does not give
a definite answer
as to whether the
pregnancy is affected or not. The
risk in this
case based on the mother’s age alone is 1 in 276,
but the high
NT measurement combined with the maternal age suggests that the risk for this particular baby is 1 in 30. Most women
even with a high risk result
actually have a normal fetus (a false-positive result).
Available options
Any
risk above 1 in 250 to 300 is considered ‘high risk’ and such women
are offered diagnostic testing
to give a definite diagnosis. Samples are obtained
by chorionic villous sampling (CVS) at 11–14 weeks
or by amniocentesis from 15 weeks. Both
involve an ultra- sound-guided needle
inserted through the abdominal wall under local
anaesthetic. Both are associated with approximately 1 in 100 risk
of procedure-related miscarriage. CVS can be performed earlier, which allows
for earlier termination if that is chosen, but
has a risk of not giving a true result (mosaicism). Amniocentesis is performed
from 15 weeks and has no risk
of placental mosaicism.
A
couple may alternatively choose to avoid
invasive testing and have a detailed anomaly scan at 20 weeks
to assess for
‘soft markers’ of Down’s syndrome (such as skull
abnormal- ities, ventriculomegaly, atrial septal defect, duodenal atresia, echogenic bowel, hydronephrosis
and short limbs).
This couple opts for amniocentesis
at 16 weeks’ gestation and the result is:
Chromosomal analysis: 46XY normal karyotype.
Further investigation
Fetuses with a high-risk NT but normal
karyotype have an increased likelihood of other structural defects
such as congenital heart disease, exomphalos, diaphragmatic hernia and skeletal defects. This couple
should therefore have a detailed
anomaly scan and fetal car- diac echo at around 20 weeks’ gestation.
Related Topics