Chapter: Case Study in Obstetrics and Gynaecology: General Obstetrics
Case Study Reports: Breech Presentation
BREECH PRESENTATION
History
You are asked
to see a woman in the antenatal clinic. She is 37 years
old and pregnant with her third child.
Her previous children were both born
by vaginal delivery after induc- tion
of labour for post dates.
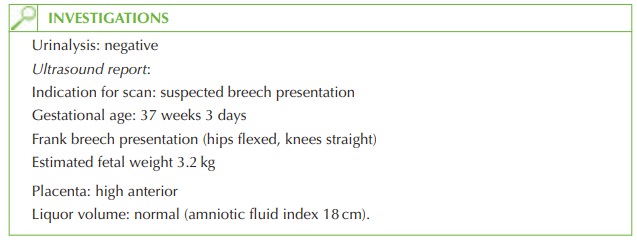
First-trimester ultrasound confirmed her menstrual dates and she is now 37 weeks.
At her last appointment at 36 weeks’
gestation, the midwife
suspected that the baby was in a breech
presentation. An appointment has been made for an ultrasound assessment and to discuss the situation.
Examination
Blood pressure is 140/85 mmHg and
abdominal examination suggests a breech presenta- tion with the sacrum not
engaged.
Questions
·
What are the options
available to the woman?
·
What management would you recommend in this case?
Answer:
At
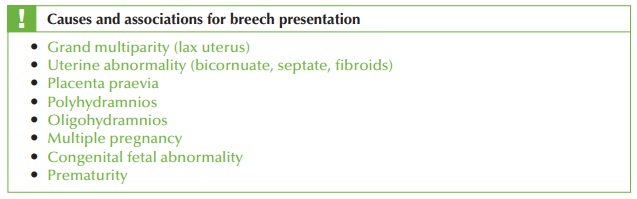
30 weeks the incidence of breech presentation is around 14 per cent,
but is only 2–4 per cent by term.
The three options available are:
·
external cephalic version
·
elective Caesarean section
·
vaginal breech delivery.
All
three options should
be discussed with the woman
and her partner
with important counselling points.
Vaginal breech delivery:
·
found to be less
safe for singleton term fetuses than
planned Caesarean section
·
carries a high chance
of necessitating an emergency Caesarean section
·
needs involvement of an experienced obstetrician with continuous fetal
heart moni- toring and
ideally an epidural
·
should only be allowed
if the labour progresses spontaneously – augmentation of breech labour is generally not recommended
·
contraindicated with placenta praevia,
large baby, footling breech
or maternal con- dition such as pre-eclampsia
External cephalic version:
·
involves using external manipulation of the fetus,
encouraging the baby to turn to
the cephalic presentation by way of pressure
on the maternal abdomen
·
is
often performed after
giving a uterine
relaxant such as salbutamol
·
carries a very small
chance of abnormal
fetal heart rate during or after the proced-
ure which could necessitate an emergency Caesarean
section
·
has
approximately 50 per cent success
rate overall
·
some fetuses revert to breech position even after successful external cephalic
version
·
contraindicated with previous Caesarean section, other uterine surgery, pre-eclampsia,
intrauterine growth retardation, oligohydramnios
·
can be painful
Elective Caesarean section:
·
is safer than vaginal breech delivery
·
is
suitable where contraindications exist to external
cephalic version
·
can
be planned for
in advance, which
women may find
more convenient
·
does not necessarily mean
a woman would
need a Caesarean section for any
future pregnancy.
In
this case the woman should
be recommended external
cephalic version as soon as pos-
sible, with options for an elective Caesarean section or possible
trial of breech
delivery if this is unsuccessful.
Postnatal paediatric review should
focus on the
baby’s hips, with
a neonatal ultrasound arranged within
6 weeks to rule out congenital hip dislocation (10–15
times more com- mon in breech presentation).
Related Topics