Chapter: Case Study in Obstetrics and Gynaecology: General Obstetrics
Case Study Reports: Diabetes in Pregnancy
DIABETES IN PREGNANCY
History
A
20-year-old woman is pregnant for the first
time. The pregnancy is unplanned and the
partner has left but she is supported by her mother
and has decided
to continue.
She
was diagnosed with type 1 diabetes aged 15 years.
She has been taking long-acting and short-acting insulin under the care of her general practitioner (GP), but the referral
letter suggests that she has not always been compliant.
She
had a positive pregnancy test
2 weeks ago
and her GP has referred her urgently to the
antenatal clinic for review in view of the diabetes. By her dates
she is now 7 weeks
and 5 days’ gestation. She has no other significant gynaecological or medical
history.
Examination
The
woman has a body mass
index of 29 kg/m2. Blood
pressure is 131/68
mmHg and pulse is 81/min.

Questions
·
What further investigations need to be arranged?
·
Outline the principles of management of the pregnancy.
Answer:
The investigations can be divided
into those for maternal and for fetal wellbeing:
·
maternal wellbeing:
·
baseline urea and electrolytes
·
pre- and post-prandial capillary
blood glucose measurements
·
fetal wellbeing:
·
viability scan (increased risk of miscarriage in diabetic women)
·
fetal echocardiography (increased risk
of all fetal
abnormalities in diabetic offspring)
·
detailed anomaly ultrasound examination at 20 weeks.
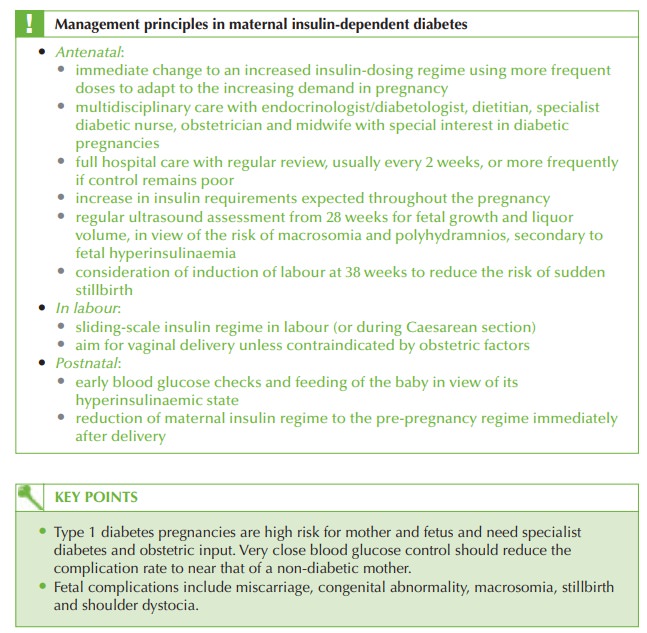
Diabetic (type 1) pregnancies may be affected
by an increase in a range of complications
as well as fetal abnormalities. However optimal control
of blood sugar is thought
to reduce the complication risk to near that of a non-diabetic pregnancy, so a large propor- tion of management is aimed at maintaining very
tight blood glucose
control. In this
par- ticular case, the history, HbA1c and presence of glycosuria suggest
that the woman
has generally poor control, providing a particular challenge to management of this pregnancy.
Related Topics