Chapter: Case Study in Obstetrics and Gynaecology: General Obstetrics
Case Study Reports: Pain in Pregnancy
PAIN IN PREGNANCY
History
A
40-year-old woman presents
with a fever and abdominal pain. She is 18 weeks
preg- nant in her
third pregnancy. The
pregnancy has been
unremarkable so far
and she has
no significant gynaecological or medical history.
She
has felt unwell for 10 days but has become worse in the last 48 h. She is nauseated and has vomited several
times. She is intermittently hot and cold.
Her abdominal pain is
generalized and constant
with some right-sided loin pain.
She
denies any dysuria
and says that she has frequency which
has been present
through- out the pregnancy. She has had no recent
change in bowel
habit. There has been no vaginal bleeding and she has a mild thin vaginal discharge.
Examination
She
appears flushed and unwell. Her temperature is 38.2°C, blood pressure 115/68 mmHg and pulse 112/min.
Cardiac and chest
examination is normal.
The fundal height
is approxi- mately 2 cm below the umbilicus, and the uterus
is soft and non-tender. The rest of the
abdomen is tender on deep palpation, maximally
in the right lower quadrant.
There is right renal
angle tenderness. The
fetal heart is heard at 160/min with
hand-held Doppler.
Questions
·
What is the diagnosis?
·
How
would you investigate and manage this woman?
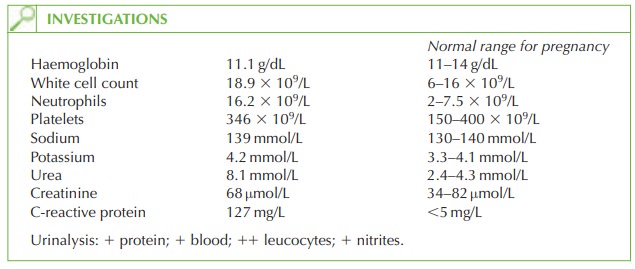
Answer:
The
diagnosis is of pyelonephritis, which occurs in 1–2 per cent of pregnancies. Women can be very unwell with non-specific symptoms. In this case specific
factors are evident (loin pain and positive urinalysis).
Urinary tract infections (UTIs) are common in pregnancy
due to progesterone causing
stasis of urine and pressure
of the gravid uterus causing
ureteric obstruction.
Further investigation
The
diagnosis should be confirmed with urine microscopy, culture and sensitivity, and blood cultures should
be sent prior
to commencing antibiotics. Renal tract ultrasound scan is necessary to rule out
any congenital abnormality (such as duplex
ureters) that may predispose to renal tract infection, and to rule out an infected obstructed kidney which could need
urgent drainage by nephrostomy. Renal
tract ultrasound, however, can be dif- ficult to interpret in pregnancy as physiological dilatation of the ureters
occurs from pres- sure from the uterus.
Management
Intravenous antibiotics should be started, usually
cephalosporins, until culture
and sensi- tivities are available, with regular paracetamol to control the temperature and pain. It may
take several days for the temperature to settle and for the woman’s pain and symptoms
to resolve, but improvement should be monitored with daily white
blood count, C-reactive protein and urea and electrolytes. Intravenous rehydration is needed as the woman is vomiting and pyrexial with raised urea,
suggesting dehydration.
After completion of treatment (total 2 weeks)
a repeat urine
culture is needed
to confirm cure. Some
women with recurrent infection need a daily prophylactic antibiotic regime.
Effect on the pregnancy
Maternal sepsis is a risk for
miscarriage and preterm
labour, so treatment should not be delayed. In addition, recurrent UTI, even asymptomatic bacteriuria, is associated with intrauterine growth retardation and preterm labour.

Related Topics