Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Excessive Hair Growth
EXCESSIVE HAIR GROWTH
History
A
19-year-old woman was referred by her general
practitioner (GP) with increased hair growth.
She
first noticed the problem when she was about 16 years old and it has progressively worsened such that she now feels
very self-conscious and will never
wear a bikini or go swimming. It also affects
her forming relationships. The hair growth
is noticed mainly
on her arms, thighs
and abdomen. Hair
has developed on the upper
lip more recently. She has tried shaving
but this seems
to make the
problem worse. She
feels depilation creams
are ineffective. Waxing is helpful but very expensive and she has bleached her upper-lip hair. Her GP has not prescribed any medication in the past.
There is no significant previous medical history
of note. Her periods started
at the age of 13 years
and she bleeds
every 30–35 days.
The periods are
not painful or heavy and
there is no intermenstrual bleeding or discharge. She has never
been sexually active.
Examination
On
examination she has
an increased body
mass index (BMI)
of 29 kg/m2. The blood
pres- sure is 118/70 mmHg.
There is excessive hair growth on the lower
arms, legs and thighs and in the midline of the abdomen
below the umbilicus. There is a small amount
of growth on the
upper lip too.
The abdomen is soft and
no masses are
palpable. Pelvic
examination is not indicated
as she is a virgin.
Questions
·
What is the likely diagnosis?
·
How
would you further
investigate and manage this woman?
ANSWER
The
likely diagnosis is of polycystic ovarian syndrome (PCOS).
This is supported by the clinical features
of hirsutism, acne,
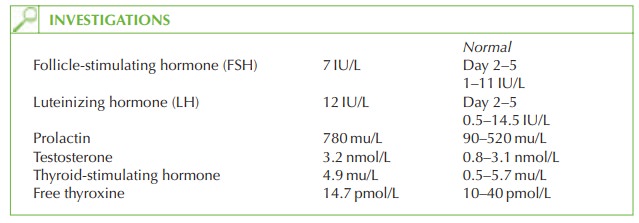
increased BMI and slight menstrual irregularity. The
biochemical results show the typical
moderately raised androgen
and raised LH to FSH ratio.
If
the testosterone level was higher,
androgen-secreting tumours should be considered (androgen-secreting ovarian,
pituitary or adrenal
tumours).
Other causes of hyperandrogenism include iatrogenic (glucocorticoids, danazol, testos-
terone), idiopathic or familial.
Further investigation
A transabdominal ultrasound scan
should be arranged to confirm the ultrasound
features of polycystic ovaries,
although this is not in fact an essential feature
for the diagnosis of the syndrome.
Treatment
Various treatments are used for hirsutism once serious causes of
hyperandrogenism have been excluded. One of the commonest is to commence
the cyproterone acetate-containing combined oral contraceptive pill (co-cyprindiol). Cyproterone acetate is an anti-androgen
with progestogenic activity. It takes several
months for an improvement to be seen in the hair
growth and she
will continue to need to use the
cosmetic treatments in the meantime.
If
this is ineffective then cyproterone acetate
at a higher dose can be used either alone,
or in addition to co-cyprindiol.
General advice should include
weight loss, as this counteracts the metabolic imbalance associated with PCOS and is favourable in the long term in terms of the known
cardio- vascular risks associated with
hyperandrogenism.
Related Topics