Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Shortness of Breath and Abdominal Pain
SHORTNESS OF BREATH AND ABDOMINAL PAIN
History
A
72-year-old woman has
been admitted with
shortness of breath.
On further questioning she says she has been unwell
for about 8 weeks. She has decreased appetite and nausea when she eats. She has lost weight but her abdomen
feels swollen. She has generalized dull abdominal pain and constipation, which
is unusual for her. There
are no urinary symptoms.
She
has always been healthy with no previous
hospital admissions. She is a widow and did
not have any children. Her periods stopped
at 52 years and she has had no post- menopausal bleeding. She has
never taken hormone-replacement therapy.
Examination
She
appears pale and breathless on talking. Chest
expansion is reduced
on the right side, with dullness to percussion and
decreased air entry
at the right
base. The abdomen
is gen- erally distended with shifting dullness. There is a mass arising
from the pelvis.
Speculum examination is normal,
but on bimanual palpation there
is a fixed left iliac
fossa mass of about 10 cm diameter.

Questions
·
What is the likely diagnosis?
·
How
should this woman
be further investigated?
·
If
the diagnosis is confirmed how should she be managed?
ANSWER
The
history and examination are suggestive of a right
pleural effusion and ascites. The presence of a pelvic
mass would suggest
that this is due to an ovarian
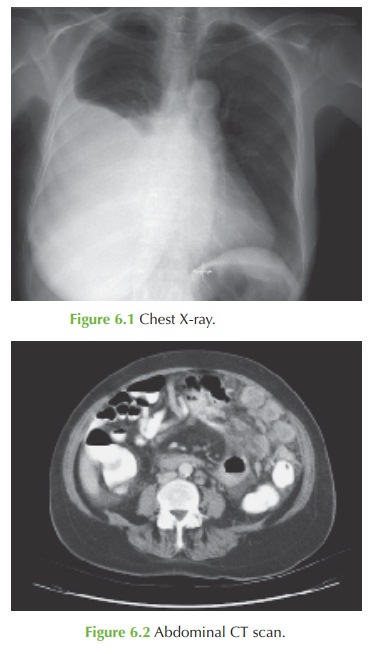
or bowel problem. The chest X-ray confirms
the effusion, and the CT shows a left-sided pelvic
tumour and ascites. There
are also solid
areas in the anterior abdominal wall that represent omental infiltration by the
tumour.
CA-125 is a non-specific marker for ovarian
carcinoma. The diagnosis is therefore likely to be that of ovarian cancer which commonly
presents with systemic
symptoms when metastatic
disease is already evident.
Confirmation of the diagnosis and management
The
surgical aphorism ‘there
is no diagnosis without a surgical diagnosis’ means that tis- sue
needs to be obtained to confirm the diagnosis. Laparotomy should be performed with three objectives:
·
obtaining tissue for diagnosis
·
staging the disease according to the extent
of tissue involvement
·
primary debulking – to perform a total abdominal hysterectomy and bilateral salping- oophorectomy and to reduce all abdominal tumour
deposits to a volume of less than 2
cm. This allows
optimal effect of chemotherapy following surgery. Lymph node dis-
section and omental resection are usually part of the procedure.
Prior to any treatment
this woman also needs drainage
of her pleural effusion for symp-
tomatic relief and optimization for anaesthetic.
The prognosis for ovarian cancer is
poor, as most women present at stage 3 or 4.
Related Topics