Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Pelvic Pain
PELVIC PAIN
History
A
21-year-old student presents with left iliac
fossa and lower
abdominal pain. The
pain is present intermittently and there is no pattern
to it except that it is generally worse on exercise and so she has stopped
running to keep fit. The pain started
about 6 months before and has gradually
become
more common and severe.
It is no worse with her
periods and she is not currently sexually
active so cannot report any dyspareunia. Her periods are regular and not particularly heavy or painful.
She has not had any previous
gynaecological problems. She has had one sexual partner who she was with for 4 years. She denies any sexually transmitted infections.
Medically she is fit and well,
and has only been admitted
to hospital for wisdom teeth removal and for tonsillectomy as a child.
She takes no medications.
Examination
The
woman is slim
and the abdomen
is soft with
a palpable mass
in the left
iliac fossa. This is firm and feels mobile.
It is moderately tender.
Speculum examination is normal.
Bimanual examination confirms
an 8 cm mass in the
left adnexa. The uterus is palpable separately and is mobile
and anteverted. The right
adnexa is normal.
Questions
·
What is the diagnosis?
·
How would you manage this woman?
ANSWER
The
woman has a left ovarian
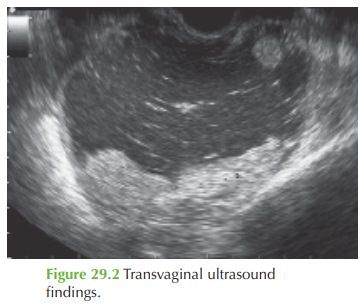
cyst. The ultrasound appearance shows an ovarian cyst.
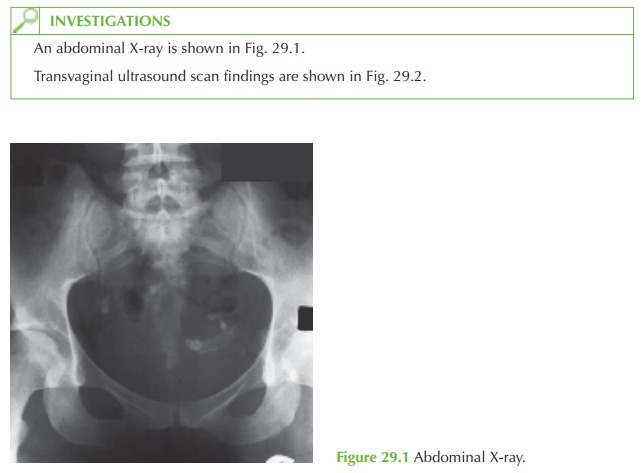
The appearance is of mixed echogenicity with ‘acoustic shadowing’ and this appearance is typical for a dermoid cyst (also known as a benign teratoma). The X-ray shows the pres- ence of teeth in the left iliac fossa region.
These cysts are common.
Typically sebaceous fluid is present,
often in association with strands of hair or sometimes teeth. If active
thyroid tissue develops
the woman may pre-
sent with features of hyperthyroidism and the cyst
is referred to as a struma ovarii.
The
management is surgical
with ovarian cystectomy, due to the size of the cyst and the symptoms. Ideally this can
be performed laparoscopically. In asymptomatic cysts
there is a possibility of expectant management (‘watch and wait’).
However the risks of leaving the cyst are:
·
malignancy occurs in up to 2 per cent of dermoid
cysts
·
ovarian torsion is thought
to be relatively common in women with dermoid cysts and if this occurs
it is a medical emergency, which may involve
oophorectomy.
The
woman should be advised that the cysts
are common and there is very little
chance that it is malignant or that removing
it will affect
her fertility. However,
recurrence may occur in either ovary
and she should
seek further consultation if she develops recur- rent pain.
Related Topics