Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Postoperative Confusion
POSTOPERATIVE CONFUSION
History
You are on call and
are asked to see a woman in the day
surgery unit who
is confused postoperatively. She is 42 years old and underwent
transcervical resection of multiple
submucosal fibroids in the early afternoon after presenting with menorrhagia.
Four fibroids were resected
and the estimated blood loss was 150 mL.
Examination
The
woman knows her
name but is disorientated, scoring
only 5/10 on a mini mental
state examination. She seems slightly
drowsy.
The
heart rate is 100/min and
the blood pressure is 105/70
mmHg. Oxygen saturation is 94 per cent
on air. She
is apyrexial. Chest
examination reveals dullness at both bases
with fine inspiratory crackles.
The abdomen is not distended
but there is generalized lower abdominal tenderness. No masses
are palpable and there are no signs
of peritonism. You can see that there
is small amount
of blood from the vagina,
but the loss is not excessive.
You
are told that she passed
urine an hour ago without
difficulty.
The
operation note is reviewed and
you find that
the procedure was
essentially uncompli- cated but
was halted before
all the fibroids could be fully
resected because of the fluid imbalance. The fluid deficit
is recorded as 1010 mL. However
you review the actual fluid chart and it is as follows:
Fluid input (glycine, via operating hysteroscope input channel): 1000 mL
1000 mL
1000 mL
950 mL
Fluid output (via operating hysteroscope output channel):
1940 mL
Questions
·
What is the diagnosis
and why has it occurred?
·
How would you manage this patient?
Answer:
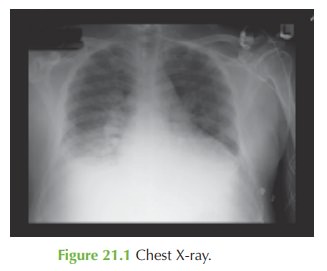
The
chest examination and X-ray suggest
pulmonary oedema. Investigations show hyponatraemia and this is a recognized cause
of a confusional state. There
is also hypokalaemia which
puts her at risk of dysrhythmia or cardiac arrest.
There has been an error in calculating the
fluid deficit such
that the deficit
is in fact 2010 mL rather than 1010 mL. The hyponatraemia is therefore caused by fluid overload,
a recognized complication of transcervical resection procedures. The
normal upper limit for the procedure is 1000 mL and in this case twice
that volume has been absorbed.
Management
The
mainstay of management is supportive with
monitoring of electrolytes and fluid
restriction. Potassium supplementation should be given and electrocardiogram (ECG) monitoring employed until the potassium
is normal.
The
woman should be transferred to a high-dependency bed and given oxygen. Arterial blood gas should be monitored, and if the pulmonary oedema
worsens then diuretics will be needed.
The
hyponatraemia usually corrects
itself with time and fluid
restriction, and the acute
confusional state would
be expected to resolve as the electrolytes normalize.
The fibroids were not completely resected and a repeat ultrasound or outpatient
hysteroscopy may be considered after a few weeks to check whether further surgery is needed
– sometimes degeneration may occur as a result
of thermal damage
or inflammation from the initial
pro- cedure. Alternatively any fibroid remnants may be expelled
spontaneously through the cervix
and vagina.
Related Topics