Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Pelvic Pain
PELVIC PAIN
History
A
29-year-old woman presents with lower abdominal pain for 4 years occurring with her periods. She takes paracetamol and ibuprofen and goes to bed with a hot water bottle for up to 2 days every
month. For the last 18 months pain has also occurred in between
periods.
The
pain is dull and constant
across the lower
abdomen. Her periods
are regular and there
is no menorrhagia, intermenstrual or postcoital bleeding. There is no other significant medical history.
She
has been married
for 2 years and has deep dyspareunia which makes her interrupt
intercourse. She does
not use any
contraception, as they
are keen to start a family. She
has never been pregnant in the past.
Examination
There is generalized lower-abdominal
tenderness, particularly in the suprapubic area but no masses are palpable. Speculum
examination is unremarkable. On bimanual palpation the uterus is axial
and fixed with cervical excitation. The pouch of Douglas is very tender and contains a mass.
The adnexae are both tender
but no adnexal masses are palpable.


Questions
·
What is the diagnosis?
·
How would you further manage this woman?
ANSWER
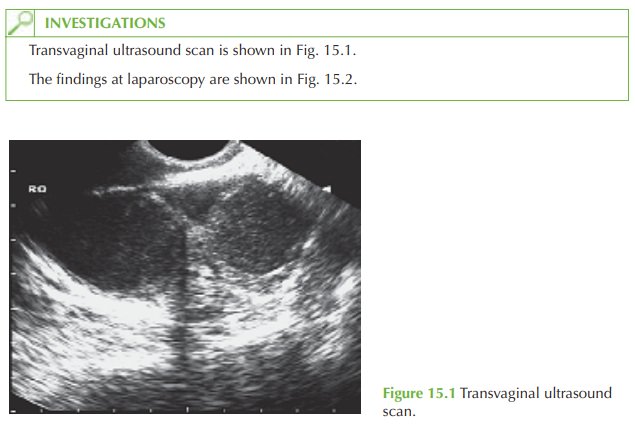
The
history of dysmenorrhoea and dyspareunia are classic for endometriosis, and the
ultrasound examination and laparoscopy images
show bilateral endometriomas (‘choc- olate cysts’), a complication of this disease.
Endometriosis is a common
condition where active
endometrial glands and stroma are located outside the endometrial cavity. Endometriomas develop
as ectopic endometrial tissue on the ovary
produces blood, which
builds up into an encapsulated cyst with each consecutive menstrual cycle.
Endometriosis is benign but carries a high physical
and psychological morbidity
due to the clinical features:
·
pelvic pain
·
dysmenorrhoea
·
dyspareunia
·
infertility.
Examination findings include tenderness or a pelvic
mass, and may
include palpable nod- ules in the rectovaginal septum and a fixed retroverted uterus secondary to adhesions (the frozen pelvis).
Diagnosis is made at laparoscopy, although
ultrasound features such as these ovarian
cysts containing ‘ground-glass’ echoes can be suggestive.
Management
The
mainstay of management for endometriosis is surgical, with ablation or excision of endometriotic deposits by laparoscopy. In this case there are bilateral endometriotic cysts that need to be removed
laparoscopically by incision
and drainage with excision of the
cyst capsules. Surgical treatment should relieve the dyspareunia and
dysmenorrhoea and may improve fertility in more severe disease.
Medical suppression of endometriosis
is possible with the contraceptive pill or gonadotrophin-releasing hormone
analogues, which inhibit
ovulation and hence
stimul- ation of endometrial deposits by oestrogen. However these are ineffective for endometri-
omas. The levonorgestrel-releasing intrauterine device has also been used to suppress endometriosis and reduce symptoms.

Related Topics