Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Amenorrhoea
AMENORRHOEA
History
A 32-year-old woman complains that she has not had a period
for 3 months. Four home pregnancy tests have all been negative. She started her periods at the age of 15 years and until 30 years she had a normal 27-day
cycle. She had one daughter
by normal delivery 2 years ago, following which she breast-fed for 6 months.
After that she had normal cycles again for several
months and then
her periods stopped
abruptly. She was
using the progesterone only
pill for contraception while she was
breast-feeding and stopped
6 months ago as she is keen to have another
child. She reports
symptoms of dryness
during intercourse and has experienced sweating
episodes at night
as well as episodes of feeling
extremely hot at any time
of day. There is no relevant gynaecological history. The
only medical history of note is that she has been hypothyroid for 10 years and takes thyroxine 100 μg per day. She does not take any alcohol,
smoke or use recreational drugs.
Examination
Examination findings are unremarkable
Questions
·
What is the diagnosis?
·
What further investigations should
be performed?
·
What are the important points in the management of this woman?
ANSWER
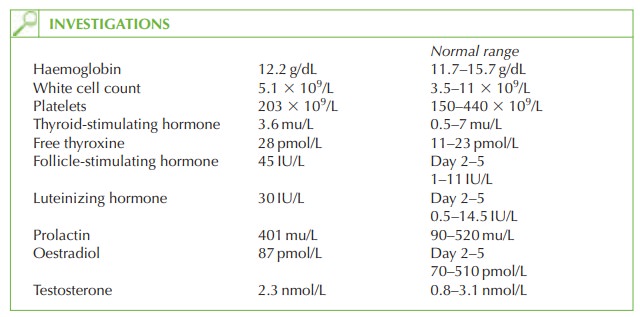
This woman has symptoms
of amenorrhoea as well as hypo-oestrogenic vasomotor symp- toms and vaginal
dryness. The diagnosis
is of premature menopause, confirmed
by the very high gonadotrophin levels.
High levels occur because the ovary is resistant to the
effects of gonadotrophins, and negative feedback to the hypothalamus and
pituitary causes increasing secretion to try and stimulate the ovary. Sheehan’s
syndrome (pituitary necrosis after postpartum haemorrhage) would also
cause amenorrhoea but
would have inhibited breast-feeding and all menstruation since delivery.
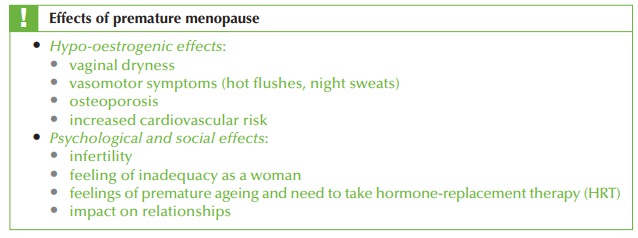
Premature menopause (before the age of 40 years)
occurs in 1 per cent of women
and has significant physical
and psychological consequences. It may be idiopathic but a familial tendency is common. In some cases
it is an autoimmune condition (associated with
hypothyroidism in this case). Disorders of the X chromosome can also be associated.
Further investigations
Repeat
gonadotrophin level is required
to confirm the result
and exclude a midcycle gonadotrophin surge or fluctuating gonadotrophins. Bone scan is necessary for baseline bone density and to help in monitoring the effects of hormone
replacement. Chromosomal analy-
sis identifies the rare cases of premature
menopause due to fragile
X syndrome or Turner’s
syndrome mosaicism.
Management
Osteoporosis may be prevented with
oestrogen replacement, with progesterone protection of the uterus. Traditional HRT preparations or the combined
oral contraceptive pill are
effective, the latter making women feel more ‘normal’, with a monthly
withdrawal bleed and a ‘young
person’s’ medication.
Her
options are adoption, accepting childlessness and in vitro
fertilization (IVF) with donor oocytes.
Occasionally premature menopause is a fluctuating
condition (resistant ovary syndrome) whereby the ovaries may function
intermittently. Contraception should therefore be used if it would be
undesirable to become pregnant.
Patient support organizations are a good source
for women experiencing such an unex- pected and stigmatizing diagnosis.
Related Topics