Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Labile Mood and Abdominal Pain
LABILE MOOD AND ABDOMINAL PAIN
History
A
37-year-old mother presents
to her general practitioner with cyclical labile mood
swings. She says that she has always
suffered with ‘PMS’
(premenstrual syndrome) and that
it is in the family
as her mother
had to have
a hysterectomy for
the same problem. She reports her periods
as always having
been painful and that she has always
been irrit- able leading
up to a period. However
now she feels
that she is not herself
for at least 2
weeks before her period and that the pain has worsened. She also notices
headaches, swelling and breast tenderness.
Her
periods are generally with regular bleeding
for up to 6 days every 27–31 days.
She has had three
children all by normal vaginal
delivery and the
youngest is now
5 years old.
She has no other medical history of note.
She
has been married
for 14 years
and she says
she often feels
aggressive towards her
hus- band or alternatively is tearful and low. Prior to having children
she worked in a bank and
is not sure whether to return as she feels she might be unable to cope.
Examination
No abnormality is found on abdominal
or neurological examination.
Questions
·
What is the differential diagnosis?
·
How
would you further
determine the cause
of the symptoms and manage
this patient?
ANSWER
The
woman clearly feels
that this is a gynaecological problem and that
she has PMS.
The diagnosis should be confirmed with evidence of symptoms occurring in the luteal
phase and resolving within
a day or two of menstruation starting. The differential diagnosis is depression which can manifest in a similar
way to PMS.
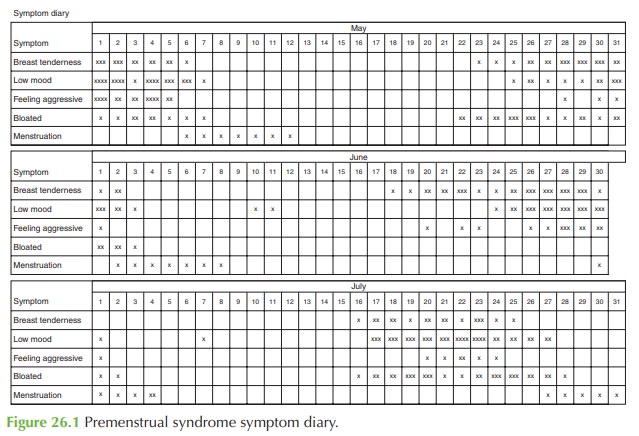
A
symptom diary is needed for recording symptoms
for each day, over a 3-month
period. The woman should annotate a chart with the severity
of each symptom and when menstruation occurs. PMS should
start after midcycle, symptoms should resolve
with the period, and there should
be a number of symptom-free days each month.
An example of a symptom diary is
shown in Fig. 26.1.
Management
If
confirmed then the diagnosis should
be discussed with the woman,
offering appropriate
understanding and support
but explaining that management is variable in the success
for each woman and that ‘one size does not fit all’. Vitamins and oil of evening primrose
are not proven in trials but may have a placebo
effect.
Interruption of ovulation with the
oral contraceptive pill is often successful in
women under the age of 35 years.
Selective serotonin reuptake inhibitors have a good success rate in randomized trials, and the woman
should be advised
that they have a specific
effect with PMS rather than just a general antidepressant effect.
Hysterectomy would not be helpful unless
the ovaries were
also removed, and
this would involve risk of significant morbidity with the need for hormone-replacement therapy afterwards which may have its own side-effects or complications.
Related Topics