Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Infertility
INFERTILITY
History
A
31-year-old woman and
her 34-year-old partner
are referred by the general
practitioner because of primary
infertility. They have been trying
to conceive for over 2 years. The woman has regular menstrual periods bleeding for 4 days every 28–30
days. Her periods are not heavy and have never
been painful. There
is no intermenstrual bleeding or dis-
charge and no postcoital bleeding. She has never
been diagnosed with
any sexually trans- mitted infections.
The
last smear was normal 1 year ago. She is a non-smoker and drinks alcohol
very occasionally.
The
partner’s only previous
medical history was an appendectomy and a course of anti- helicobacter therapy after he developed epigastric pain and was diagnosed with the infec- tion. He previously smoked
20 cigarettes per day and drank up to 28 units of alcohol per week
but has now
stopped smoking and
significantly reduced his
alcohol intake. He works
as buyer for a retail company.
The
couple have intercourse 1–4 times per week and there is no reported
sexual dysfunc- tion or pain on intercourse. They both deny recreational drug use.
Examination
On
examination the woman
has a body mass index
of 23 kg/m2. There is no hirsutism or acne. There are no signs of thyroid
disease. The abdomen
is soft and non-tender.
Speculum and bimanual palpation are unremarkable. Genital examination of the
partner is also normal.
Questions
·
How
do you interpret the investigation results?
·
Are any further investigations necessary?
·
How would you manage this couple?
Answer:
Day
21 progesterone above 30 nmol/L confirms
ovulation, and this is supported by nor- mal follicle-stimulating hormone
(FSH), luteinizing hormone
(LH) and prolactin. Normal testosterone suggests that polycystic ovaries
is an unlikely diagnosis.
The
semen analysis is normal, and therefore any male factor
aetiology is unlikely. Rubella immunity should always be confirmed.
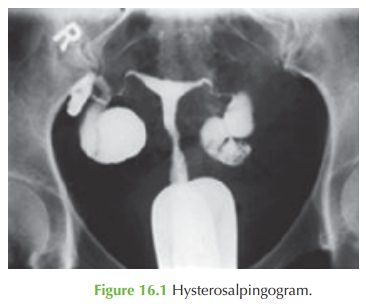
The
hysterosalpingogram shows fill of contrast
medium into both uterine tubes
but no spill, suggesting tubal obstruction as the cause
of the fertility problem.
Further investigations
Tubal blockage on hysterosalpinogram can
sometimes be due
to tubal spasm,
and there- fore a laparoscopy and
dye is needed
to confirm the
pathology and also
to determine a cause
such as adhesions from previous infection or possibly endometriosis (although the
history does not support this diagnosis).
Management
If
the tubes are found at dye test to be patent, then this would
suggest that it is feasible
to attempt pregnancy with in utero
insemination. However if blocked tubes
are confirmed then in vitro fertilization (IVF) is indicated. Abnormal tubes are usually removed
prior to IVF, as success
rates for pregnancy are better and
ectopic pregnancy rate
reduced after bilateral salpingectomy.
General advice should be given to take folic
acid 400 μg daily to reduce the risk of neural
tube defects, and to the partner to minimize his alcohol intake.
In
this case the
laparoscopy showed bilateral hydrosalpinges and
adhesions as well as peri- hepatic ‘violin-string’ adhesions. These
findings are consistent with previous infection with chlamydia (or more rarely gonorrhoea). It is not unusual to find such severe pelvic adhesions even when there
has never been a clear
clinical history of pelvic infection or sexually transmitted infection. Although the infection may be long ago, it is sensible
to treat both the
woman and her
partner with a course of antibiotics for
pelvic inflammatory disease.
Related Topics