Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Infertility
INFERTILITY
History
A 31-year-old woman
has been trying
to conceive for
nearly 3 years
without success. Her last period started 7 months ago
and she has
been having periods
sporadically for about 5
years. She bleeds
for 2–7 days and the periods occur
with an interval
of 2–9 months. There is no dysmenorrhoea but occasionally the bleeding is heavy.
She was pregnant
once before at the age of 19 years and had a termination of pregnancy.
She had a laparoscopy several
years ago for pelvic pain,
which showed a normal pelvis.
Cervical smears have always been normal and there is no history
of sexually transmitted infection.
The woman was diagnosed with irritable bowel
syndrome when she was 25, after thor- ough investigation for other bowel
conditions. She currently uses metoclopramide to increase gut motility, and antispasmodics.
Her partner is fit and well, and has two children by a previous
relationship. Neither part- ner drinks alcohol or smokes.
Questions
·
What is the diagnosis and its aetiology?
·
How
would you further
investigate and manage this couple?
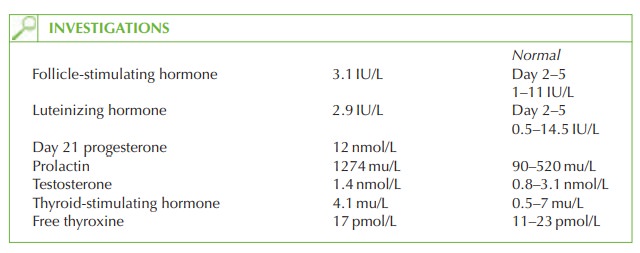
The infertility is secondary to
anovulation as shown by the day 21 progesterone
(>30 nmol/L suggests ovulation has occurred). Normal testosterone and
gonadotrophins and high prolactin suggest the likely case of anovulation is hyperprolactinaemia. Hyperprolactinaemia may
be physiological in breast-feeding, pregnancy and stress. The commonest causes of pathological
hyperprolactinaemia are tumours and idiopathic hypersecretion, but it may also be due to drugs,
hypothyroidism, ectopic prolactin secretion
or chronic renal
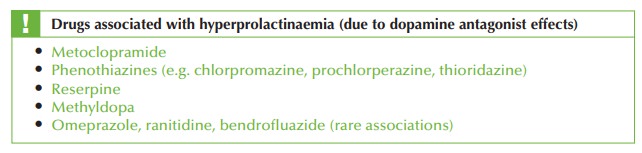
failure. In this
case the metoclopramide is the cause,
as it is a dopamine antagonist (dopamine usually acts via the hypothalamus to cause inhibition of prolactin
secretion, and if this is interrupted, prolactin is excreted to excess). Galactorrhoea is not a common
symptom of hyperprolactinaemia, occurring in less than
half of affected women.
The
metoclopramide should be stopped and
the woman reviewed after 4–6 weeks
to ensure that the periods have restarted and that the prolactin level
has returned to normal.
If this does not occur,
then further investigation is needed to exclude other
causes of
hyperprolactinaemia such as a pituitary micro- or macro-adenoma. It would be advisable
to repeat the day 21 progesterone level to confirm
ovulatory cycles. The woman should have her rubella immunity checked and should
be advised to take preconceptual folic acid until
12 weeks of pregnancy.
If the woman
fails to conceive
then a full fertility investigation should be planned
with semen analysis and
tubal patency testing
(hysterosalpingogram or laparoscopy and dye test).
Related Topics