Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Amenorrhoea
AMENORRHOEA
History
A
14-year-old girl is seen by her general
practitioner because her mother is worried that her
periods have not
started. Her older
sister started at 13 years
and her younger
sister has just started
her periods at 12 years,
and she is now embarrassed at school as her friends are always discussing their
periods and she
has not told
them that she
has not had
one.
Her
mother is also concerned because
she has not developed pubic
and axillary hair or
breast enlargement.
She
was born at 38 weeks
by spontaneous vaginal
delivery and has never had any par- ticular medical problems. She reached all her developmental milestones as a child although has not started a teenage growth
spurt and is the second
shortest girl in her class.
She
eats normally with her family
and denies any eating disorder. She takes part in school sport but does not exercise to excess.
She is sociable with her friends but
has never had a boyfriend.
Her
school academic performance is about average,
although she does not do as well as
her siblings who are all in the top streams
of their years.
Examination
On
examination she is 120 cm and weighs
59 kg. She has no abnormal facial
features but has a wide carrying
angle (cubitus valgus)
and a wide neck. There is no apparent breast development and the nipples
appear widely spaced.
No axillary hair growth is apparent.
Abdominal examination is unremarkable. The external genitalia
are normal though no
pubic hair is visible. Internal
examination is not performed.
Questions
·
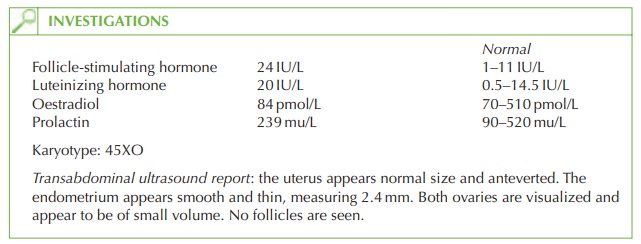
What is the most likely diagnosis
and how might this be confirmed?
·
What are the principles of management for this girl?
Answer:
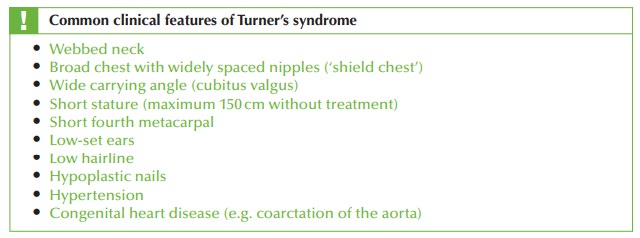
The
clinical features are typical of those of Turner’s syndrome. This genetic condition is associated with the
absence of one
X chromosome (XO
karyotype), occurring in approxi-
mately 1 in 2500 live
female births. It is confirmed on chromosomal analysis.
In
rare cases it may occurs
as a mosaic form (XX/XO),
in which case the features
are milder and the woman may start menstruating but then experience premature ovarian
failure and secondary amenorrhoea.
Management
Management of Turner’s syndrome should be carried
out in a specialist referral centre.
·
Psychological: the implications
of Turner’s syndrome diagnosis are devastating for the child and for the family.
The absence of periods may be stigmatizing and the long-term lack of fertility is a very serious concept
that may be difficult for a young girl to comprehend.
·
Medical:
·
the
short stature should
be treated to enable the girl to reach her full height
poten- tial. Human growth
hormone is given
to achieve this.
·
oestrogen therapy initially with ethinyl estradiol enables secondary sexual
charac- teristics of breast
development and pubic
and axillary hair to develop.
Cyclical progestogens are added
later to induce
a withdrawal bleed
(‘period’) for social
rea- sons and to protect the endometrium from hyperplasia or malignancy in the long term. Some form of oestrogen therapy
then needs to be continued until the time
of natural menopause (ideally
50 years) to prevent early-onset osteoporosis in this girl.
·
Fertility: fertility options are available with ovum donation
and hormonal support.
Related Topics