Chapter: Ophthalmology: Cornea
Refractive Corneal Procedures
Refractive Corneal Procedures
Photorefractive Keratectomy (Fig. 5.18d)
Principle: Tissue is ablatedto change the corneal curvature and to achieve arefractive
correction. Flattening the corneal
curvature corrects myopia, whereas steepening the curvature corrects hyperopia. The amount of
tissue removed at different sites can be varied with layer-by-layer excimer
laser ablation and the use of apertures. This makes it possible to correct for
myopia, by removing more tissue from the center of the cornea, or for
hyperopia, by removing more tissue from the periphery.

Indications: Best results are achieved in correcting myopia of less than
6diopters. At present stable correction can be achieved in 85 – 95% of all
cases of myopia up to !6 diopters, with deviation of !1 diopter from the target within one year. Correction of
hyperopia has also been attempted.
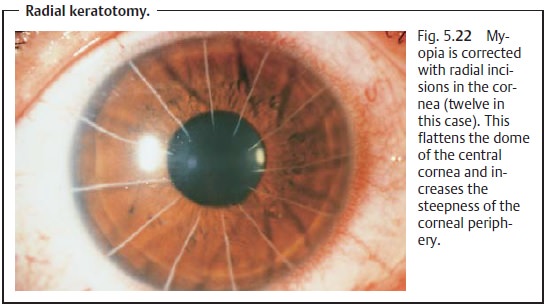
Radial Keratotomy (Fig. 5.18e)
Principle: Correction of myopia byflattening
the central dome of the corneawith four to sixteen radial incisions
extending through as much as 90% of the thickness of the cornea. This increases
the steepness of the corneal periphery and lowers the center of the cornea,
reducing its refractive power. This method does not influence the optical
center of the cornea (Fig. 5.22).
Indications and prognosis: The method is suitable for moderate myopia(less than 6 diopters). The effect achieved is influenced by the initial refrac-tion, intraocular pressure, corneal thickness, and the patient’s age and sex. A disadvantage is refractive fluctuations of up to 1.5 diopters during the course of the day. In one-fifth of all cases refraction becomes unstable within a year.
Photorefractive Keratectomy Correction of Astigmatism
Principle: Surgicalreduction of
severe regular astigmatismby flattening thesteep meridian in the center of
the cornea by increasing the steepness of the corneal periphery. Irregular astigmatism cannot be
corrected.
Indication: Severeregularastigmatism.
Holmium Laser Correction of Hyperopia
Principle: The laser is focused on the corneal stroma to create
shrinkageeffects. Placing these areas symmetrically steepens the central
cornea, which can correct severe hyperopia.
Indication: Hyperopia correction up to 8 diopters.
Epikeratophakic Keratoplasty (Epikeratophakia)
Principle: Severe myopia and hyperopia are corrected by suturing
speciallyprepared hyperopic or myopic partial-thickness corneal grafts on to
the recipient’s cornea. This involves special trephination and preparation of
the recipient’s cornea. The donor graft is then fitted into the prepared cornea
and sutured in place. The donor corneal button is prepared as a frozen section and
shaped to the required refractive power; these implants can be ordered from eye
banks.
Indications: Any severity of hyperopia or myopia can be corrected.
Excimer Laser in situ Keratomileusis (LASIK)
Principle: Myopia is corrected with preservation of Bowman’s layer. A
super-ficial corneal flap (approx. 160 µm) is created with
a microkeratome. The ker-atome is withdrawn, the flap is reflected, and the
exposed underlying corneal stroma is ablated with an excimer laser to correct
the myopia. Then the flap is repositioned on the corneal bed and fixed in place
by force of its own adhe-sion.
Indication: Even severe myopia (up to 10 – 12 diopters) can be corrected
withthis method.
Related Topics