Chapter: Basic & Clinical Pharmacology : Antihypertensive Agents
Antihypertensive Agents
Antihypertensive
Agents
Hypertension
is the most common cardiovascular disease. In a survey carried out in
2007/2008, hypertension was found in 29% of American adults. The prevalence
varies with age, race, educa-tion, and many other variables. According to some
studies, 60–80% of both men and women will develop hypertension by age 80.
Sustained arterial hypertension damages blood vessels in kidney, heart, and
brain and leads to an increased incidence of renal failure, coronary disease,
heart failure, stroke, and dementia. Effective pharmacologic lowering of blood
pressure has been shown to prevent damage to blood vessels and to substantially
reduce morbidity and mortality rates. Unfortunately, several sur-veys indicate
that only one third to one half of Americans with hypertension have adequate
blood pressure control. Many effec-tive drugs are available. Knowledge of their
antihypertensive mechanisms and sites of action allows accurate prediction of
effi-cacy and toxicity. As a result, rational use of these agents, alone or in
combination, can lower blood pressure with minimal risk of serious toxicity in
most patients.
CASE STUDY
A 35-year-old man presents with a blood pressure of 150/95Hg. He has been generally healthy, is sedentary, drinks several cocktails per day, and does not smoke cigarettes. He has a family history of hypertension, and his father died of a myocardial infarction at age 55. Physical examination is remarkable only for moderate obesity. Total cholesterol is 220, and high-density lipoprotein (HDL) cholesterol level is 40 mg/dL. Fasting glucose is 105 mg/dL. Chest x-ray is nor-mal. Electrocardiogram shows left ventricular enlargement. How would you treat this patient?
CASE STUDY ANSWER
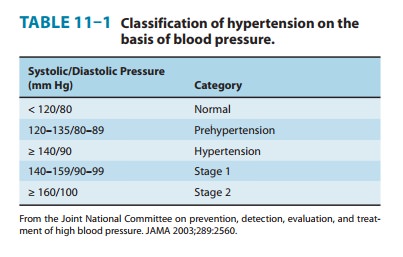
The patient has JNC stage 1 hypertension (see
Table 11-1). The first question in management is how urgent is it to treat the
hypertension. Cardiovascular risk factors in this man include family history of
early coronary disease and elevated cholesterol. Evidence of end-organ impact
includes left ven-tricular enlargement on EKG. The strong family history
sug-gests that this patient has essential hypertension. However, the patient
should undergo the usual screening tests includ-ing renal function, thyroid
function, and serum electrolyte measurements. An echocardiogram should also be
consid-ered to determine whether the patient has left ventricular hypertrophy
secondary to valvular or other structural heart disease as opposed to
hypertension.Initial management in this patient can be behavioral, including
dietary changes and aerobic exercise. However, most patients like this will
require medication. Thiazide diuretics in low doses are inexpensive, have
relatively few side effects, and are effective in many patients with mild
hypertension. Other first-line agents include angiotensin-converting enzyme
inhibitors and calcium channel blockers. Beta blockers might be considered if the
patient had coro-nary disease or had labile hypertension. A single agent should
be prescribed and the patient reassessed in a month. If a second agent is
needed, one of the two agents should be a thiazide diuretic. Once blood
pressure is controlled, patients should be followed periodically to reinforce
the need for compliance with both lifestyle changes and medications.
Related Topics