Chapter: Basic & Clinical Pharmacology : Antihypertensive Agents
Adrenergic Neuron-Blocking Agents
ADRENERGIC NEURON-BLOCKING AGENTS
These
drugs lower blood pressure by preventing normal physio-logic release of
norepinephrine from postganglionic sympathetic neurons.
Guanethidine
In
high enough doses, guanethidine can produce profound sym-pathoplegia. The resulting
high maximal efficacy of this agent made it the mainstay of outpatient therapy
of severe hypertension for many years. For the same reason, guanethidine can
produce all of the tox-icities expected from “pharmacologic sympathectomy,”
including marked postural hypotension, diarrhea, and impaired ejaculation.
Because of these adverse effects, guanethidine is now rarely used.
Guanethidine
is too polar to enter the central nervous system.
Guanadrel is a guanethidine-like drug that is available
in the USA. Bethanidine and debrisoquin, antihypertensive agents
not available for clinical use in the USA, are similar.
A. Mechanism and Sites of Action
Guanethidine
inhibits the release of norepinephrine from sympa-thetic nerve endings (see
Figure 6–4). This effect is probably responsible for most of the sympathoplegia
that occurs in patients. Guanethidine is transported across the sympathetic
nerve mem-brane by the same mechanism that transports norepinephrine itself
(NET, uptake 1), and uptake is essential for the drug’s action. Once
guanethidine has entered the nerve, it is concentrated in transmitter vesicles,
where it replaces norepinephrine. Because it replaces norepinephrine, the drug
causes a gradual depletion of norepinephrine stores in the nerve ending.
Because
neuronal uptake is necessary for the hypotensive activ-ity of guanethidine,
drugs that block the catecholamine uptake process or displace amines from the
nerve terminal block its effects. These
include cocaine, amphetamine, tricyclic antidepressants, phenothiazines, and
phenoxybenzamine.
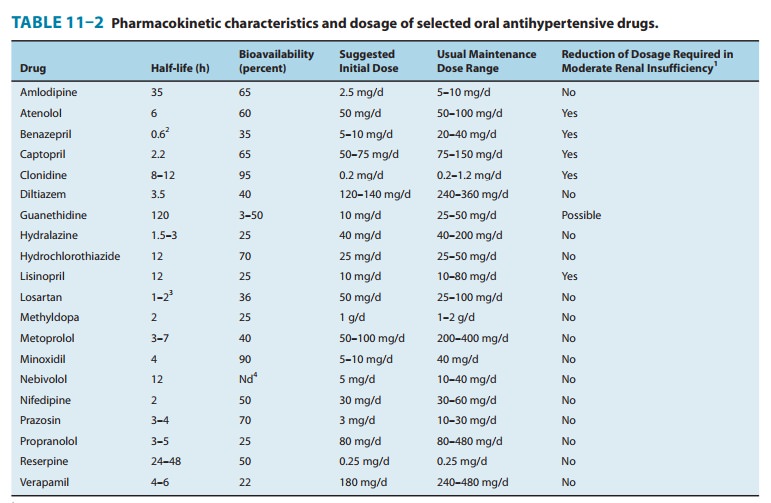
B. Pharmacokinetics and Dosage
Because
of guanethidine’s long half-life (5 days), the onset of sym-pathoplegia is
gradual (maximal effect in 1–2 weeks), and sym-pathoplegia persists for a
comparable period after cessation of therapy. The dose should not ordinarily be
increased at intervals shorter than 2 weeks.
C. Toxicity
Therapeutic
use of guanethidine is often associated with symp-tomatic postural hypotension
and hypotension following exercise, particularly when the drug is given in high
doses. Guanethidine-induced sympathoplegia in men may be associated with
delayed or retrograde ejaculation (into the bladder). Guanethidine com-monly
causes diarrhea, which results from increased gastrointesti-nal motility due to
parasympathetic predominance in controlling the activity of intestinal smooth
muscle.
Interactions
with other drugs may complicate guanethidine therapy. Sympathomimetic agents,
at doses available in over-the-counter cold preparations, can produce
hypertension in patients taking guanethidine. Similarly, guanethidine can
produce hyper-tensive crisis by releasing catecholamines in patients with
pheo-chromocytoma. When tricyclic antidepressants are administered to patients
taking guanethidine, the drug’s antihypertensive effect is attenuated, and
severe hypertension may follow.
Reserpine
Reserpine,
an alkaloid extracted from the roots of an Indian plant, Rauwolfia serpentina, was one of the first effective drugs used on
alarge scale in the treatment of hypertension. At present, it is rarely used
owing to its adverse effects.
A. Mechanism and Sites of Action
Reserpine
blocks the ability of aminergic transmitter vesicles to take up and store
biogenic amines, probably by interfering with the vesicular membrane-associated
transporter (VMAT, see Figure 6–4). This effect occurs throughout the body,
resulting in depletion of norepinephrine, dopamine, and serotonin in both
central and peripheral neurons. Chromaffin granules of the adrenal medulla are
also depleted of catecholamines, although to a lesser extent than are the
vesicles of neurons. Reserpine’s effects on adrenergic vesicles appear
irreversible; trace amounts of the drug remain bound to vesicular membranes for
many days.
Depletion
of peripheral amines probably accounts for much of the beneficial
antihypertensive effect of reserpine, but a central component cannot be ruled
out. Reserpine readily enters the brain, and depletion of cerebral amine stores
causes sedation, mental depression, and parkinsonism symptoms.
At
lower doses used for treatment of mild hypertension, reser-pine lowers blood
pressure by a combination of decreased cardiac output and decreased peripheral
vascular resistance.
Pharmacokinetics and Dosage
Toxicity
At
the low doses usually administered, reserpine produces little postural
hypotension. Most of the unwanted effects of reserpine result from actions on
the brain or gastrointestinal tract. High doses of reserpine characteristically
produce sedation, lassitude, nightmares, and severe mental depression;
occasionally, these occur even in patients receiving low doses (0.25 mg/d).
Much less frequently, ordinary low doses of reserpine produce extrapyramidal
effects resembling Parkinson’s disease, probably as a result of dopamine
depletion in the corpus striatum. Although these central effects are uncommon,
it should be stressed that they may occur at any time, even after months of
uneventful treatment. Patients with a history of mental depression should not
receive reserpine, and the drug should be stopped if depres-sion
appears.Reserpine rather often produces mild diarrhea and gastrointes-tinal
cramps and increases gastric acid secretion. The drug should not be given to
patients with a history of peptic ulcer.
Related Topics