Chapter: Basic & Clinical Pharmacology : Antihypertensive Agents
Prazosin & Other Alpha1 Blockers
PRAZOSIN & OTHER ALPHA1
BLOCKERS
Mechanism & Sites of Action
Prazosin,
terazosin, and doxazosin produce most of their antihy-pertensive effects by
selectively blocking α1 receptors in arterioles and venules. These
agents produce less reflex tachycardia when lowering blood pressure than do
nonselective α
antagonists such as phentolamine. Alpha1-receptor selectivity allows
norepineph-rine to exert unopposed negative feedback (mediated by presynap-tic α2 receptors) on its own
release ; in contrast, phentolamine blocks both presynaptic and postsynaptic α receptors, with the
result that reflex activation of sympathetic neurons by phentolamine’s effects
produces greater release of transmitter onto receptors and correspondingly
greater cardioacceleration. Alpha blockers reduce arterial pressure by dilating
both resistance and capacitance vessels. As expected, blood pressure is reduced
more in the upright than in the supine position. Retention of salt and water
occurs when these drugs are administered with-out a diuretic. The drugs are
more effective when used in combi-nation with other agents, such as a β blocker and a
diuretic, than when used alone. Owing to their beneficial effects in men with
prostatic hyperplasia and bladder obstruction symptoms, these drugs are used
primarily in men with concurrent hypertension and benign prostatic hyperplasia.
Pharmacokinetics & Dosage
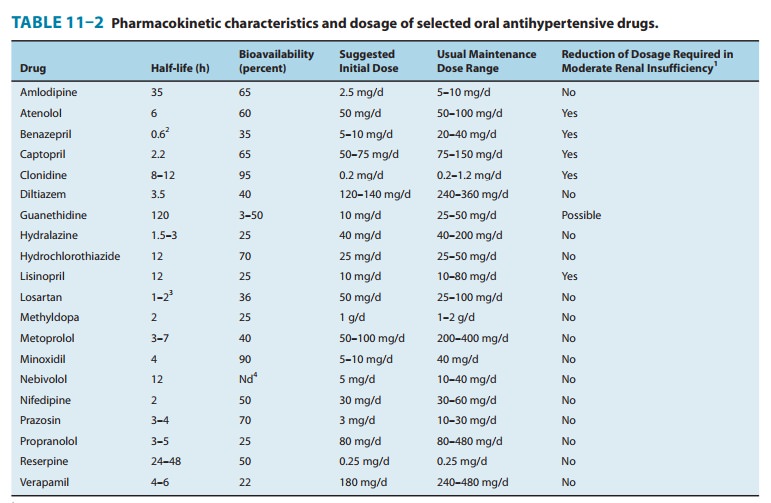
Pharmacokinetic
characteristics of prazosin are listed in Table 11–2. Terazosin is also
extensively metabolized but undergoes very littlefirst-pass metabolism and has
a half-life of 12 hours. Doxazosin has an intermediate bioavailability and a
half-life of 22 hours.Terazosin can often be given once daily, with doses of
5–20 mg/d. Doxazosin is usually given once daily starting at 1 mg/d and
progressing to 4 mg/d or more as needed. Although long-term treatment with
these α
blockers causes relatively little postural hypotension, a precipitous drop in
standing blood pressure devel-ops in some patients shortly after the first dose
is absorbed. For this reason, the first dose should be small and should be
administered at bedtime. Although the mechanism of this first-dose phe-nomenon
is not clear, it occurs more commonly in patients who are salt- and
volume-depleted.Aside from the first-dose phenomenon, the reported toxicities
of the α1 blockers are relatively infrequent and mild. These include
dizziness, palpitations, headache, and lassitude. Some patients develop a
positive test for antinuclear factor in serum while on prazosin therapy, but
this has not been associated with rheumatic symptoms. The α1 blockers do not
adversely and may even beneficially affect plasma lipid profiles, but this
action has not been shown to confer any benefit on clinical outcomes.
OTHER ALPHA-ADRENOCEPTOR– BLOCKING AGENTS
The
nonselective agents, phentolamine
and phenoxybenzamine, are useful in
diagnosis and treatment of pheochromocytoma and in other clinical situations
associated with exaggerated release of catecholamines (eg, phentolamine may be
combined with propra-nolol to treat the clonidine withdrawal syndrome,
described previously).
Related Topics