Chapter: Case Study in Obstetrics and Gynaecology: General Gynaecology
Case Study Reports: Heavy Periods
HEAVY PERIODS
History
A
39-year-old woman complains of increasingly long and heavy
periods over the last
5 years. Previously she bled for 4 days but now bleeding
lasts up to 10 days. The periods
still occur every 28 days.
She experiences intermenstrual bleeding between most
periods but no postcoital bleeding.
The
periods were never painful previously but in recent months have become extremely painful with intermittent cramps.
She has had four normal deliveries and had a laparo-
scopic sterilization after
her last child.
Her smear tests
have always been
normal, the most recent being 4 months
ago. She has never had any previous
irregular bleeding or any
other gynaecological problems.
Examination
The
abdomen is soft and non-tender with no palpable
masses. Speculum examination shows a normal cervix.
On bimanual palpation the uterus is bulky (approximately 8 week size), mobile
and anteverted. There
are no adnexal masses.
Questions
·
What is the diagnosis?
·
How
would you manage this patient
and counsel her about the management and its
potential risks?
Answer:
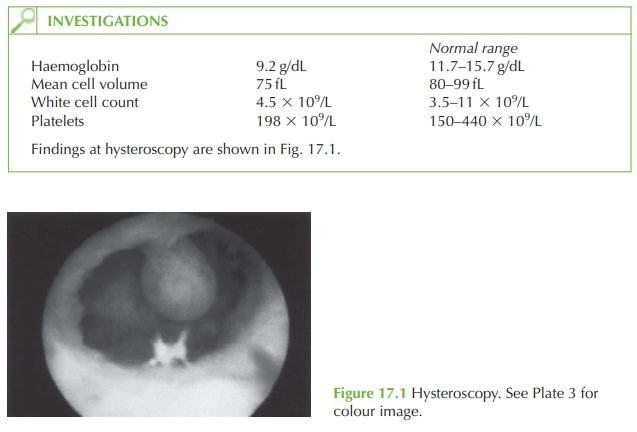
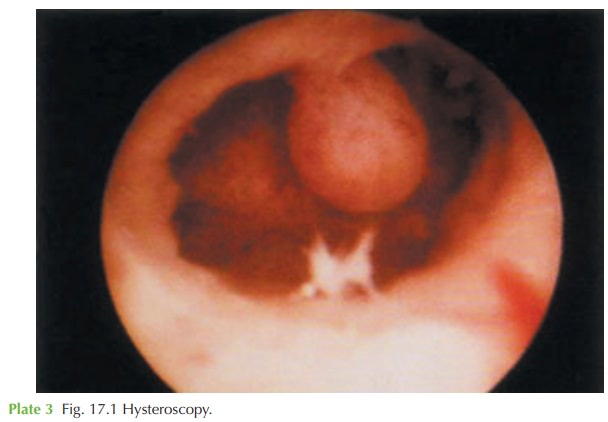
The
ultrasound scan shows a submucosal fibroid and this is confirmed
by the hysteroscopy image. At hysteroscopy, a fibroid is a solid smooth immobile
structure, whereas a polyp
appears pink and fleshy
and mobile. Submucosal fibroids are a common cause of menorrha-
gia and can cause, as in this case, intermenstrual bleeding. The cramp-like pain occurs as the
uterus tries to expel the
fibroid. In some
cases this eventually occurs with the
fibroid becoming pedunculated and extending through
to the vagina on a pedicle.
Management
The
management is by hysteroscopic (transcervical) resection of the
fibroid (TCRF). This can be performed as a day
case under general
anaesthetic (or even
local anaesthetic if the
fibroid is small). The important points in counselling the patient are as follows.
Description of the procedure: the procedure involves
stretching (dilatation) of the
cervix and insertion of an endoscope into the uterus
(hysteroscopy) to view the fibroid.
The fibroid is ‘shaved’ away with a hot wire loop (diathermy). Fluid is circulated through the uterine
cavity to enhance
the view and allow cooling.
What are the risks?
·
bleeding: it is rare to bleed
heavily but in the extreme
situation blood transfusion could be required, or even a hysterectomy to control the loss
·
infection
·
fluid overload: during the procedure, irrigation fluid is absorbed
into the circula- tion. Excessive absorption can
cause breathing difficulties (pulmonary oedema) and the need for hospital admission
·
uterine perforation: rarely the
hysteroscope perforates the
wall of the
uterus and if this
occurs or is suspected then laparoscopy is needed immediately to confirm it, secure any bleeding and
check for damage
to surrounding bowel
or bladder.
What to expect
afterwards:
most women experience bleeding, discharge and
passing of ‘debris’ for up to 2 weeks
after the procedure.
Related Topics