Chapter: Basic & Clinical Pharmacology : Antiseizure Drugs
Primidone
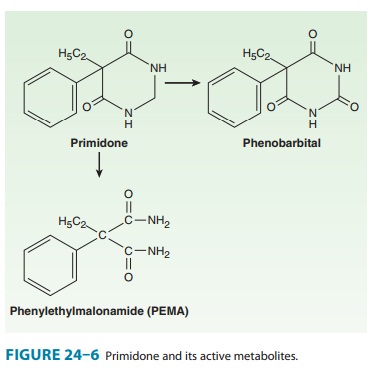
PRIMIDONE
Primidone,
or 2-desoxyphenobarbital (Figure 24–6), was first marketed in the early 1950s.
It was later reported that primidone was metabolized to phenobarbital and
phenylethylmalonamide (PEMA). All three compounds are active anticonvulsants.
Mechanism of Action
Although
primidone is converted to phenobarbital, the mechanism of action of primidone
itself may be more like that of phenytoin.
Clinical Uses
Primidone,
like its metabolites, is effective against partial seizures and generalized
tonic-clonic seizures and may be more effective than phenobarbital. It was
previously considered to be the drug of choice for complex partial seizures,
but later studies of partial sei-zures in adults strongly suggest that
carbamazepine and phenytoin are superior to primidone. Attempts to determine
the relative potencies of the parent drug and its two metabolites have been
conducted in newborn infants, in whom drug-metabolizing enzyme systems are very
immature and in whom primidone is only slowly metabolized. Primidone has been
shown to be effec-tive in controlling seizures in this group and in older
patients beginning treatment with primidone; older patients show seizure
control before phenobarbital concentrations reach the therapeutic range. Finally,
studies of maximal electroshock seizures in animals suggest that primidone has
an anticonvulsant action independent of its conversion to phenobarbital and
PEMA (the latter is relatively weak).
Pharmacokinetics
Primidone
is completely absorbed, usually reaching peak concen-trations about 3 hours
after oral administration, although consid-erable variation has been reported.
Primidone is generally distributed in total body water, with a volume of
distribution of 0.6 L/kg. It is not highly bound to plasma proteins;
approximately 70% circulates as unbound drug.
Primidone
is metabolized by oxidation to phenobarbital, which accumulates very slowly,
and by scission of the heterocyclic ring to form PEMA (Figure 24–6). Both
primidone and pheno-barbital also undergo subsequent conjugation and excretion.
Primidone
has a larger clearance than most other antiseizure drugs (2 L/kg/d),
corresponding to a half-life of 6–8 hours. PEMA clearance is approximately half
that of primidone, but phenobarbital has a very low clearance (see Table 3–1).
The appearance of phenobarbital corresponds to the disappearance of primidone.
Phenobarbital therefore accumulates very slowly but eventually reaches
therapeutic concentrations in most patients when therapeutic doses of primidone
are administered. During chronic therapy, phenobarbital levels derived from
primidone are usually two to three times higher than primidone levels.
Therapeutic Levels & Dosage
Primidone
is most efficacious when plasma levels are in the range of 8–12 mcg/mL. Concomitant
levels of its metabolite, pheno-barbital, at steady state usually vary from 15
to 30 mcg/mL. Dosages of 10–20 mg/kg/d are necessary to obtain these levels. It
is very important, however, to start primidone at low doses and gradually
increase over days to a few weeks to avoid prominent sedation and
gastrointestinal complaints. When adjusting doses of the drug, it is important
to remember that the parent drug reaches steady state rapidly (30–40 hours),
but the active metabo-lites phenobarbital (20 days) and PEMA (3–4 days) reach
steady state much more slowly.
Toxicity
The
dose-related adverse effects of primidone are similar to those of its
metabolite, phenobarbital, except that drowsiness occurs early in treatment and
may be prominent if the initial dose is too large. Gradual increments are
indicated when starting the drug in either children or adults.
Related Topics