Chapter: Basic & Clinical Pharmacology : Antiseizure Drugs
Gabapentin & Pregabalin
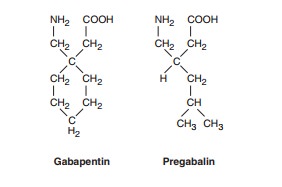
GABAPENTIN & PREGABALIN
Gabapentin
is an amino acid, an analog of GABA, that is effective against partial
seizures. Originally planned as a spasmolytic, it was found to be more
effective as an antiseizure drug. Pregabalin is another GABA analog, closely
related to gabapentin. This drug has been approved for both antiseizure activity
and for its analgesic properties.
Mechanism of Action
In
spite of their close structural resemblance to GABA, gabapentin and pregabalin
do not act directly on GABA receptors. They may, however, modify the synaptic
or nonsynaptic release of GABA. An increase in brain GABA concentration is
observed in patients receiving gabapentin. Gabapentin is transported into the
brain by the L-amino acid transporter. Gabapentin and pregabalin bind avidly to
the α2δ subunit of voltage-gated Ca2+
channels. This appears to underlie the main mechanism of action, which is
decreasing Ca2+ entry, with a predominant effect on presynaptic
N-type channels. A decrease in the synaptic release of glutamate provides the
antiepileptic effect.
Clinical Uses
Gabapentin
is effective as an adjunct against partial seizures and generalized
tonic-clonic seizures at dosages that range up to 2400 mg/d in controlled
clinical trials. Open follow-up studies permitted dosages up to 4800 mg/d, but
data are inconclusive on the effectiveness or tolerability of such doses.
Monotherapy studies also document some efficacy. Some clinicians have found
that very high dosages are needed to achieve improvement in seizure control.
Effectiveness in other seizure types has not been well demonstrated. Gabapentin
has also been promoted for the treatment of neuro-pathic pain and is now
indicated for postherpetic neuralgia in adults at doses of 1800 mg and above.
The most common adverse effects are somnolence, dizziness, ataxia, headache,
and tremor.
Pregabalin
is approved for the adjunctive treatment of partial seizures, with or without
secondary generalization; controlled clinical trials have documented its
effectiveness. It is available only in oral form, and the dosage ranges from
150 to 600 mg/d, usually in two or three divided doses. Pregabalin is also
approved for use in neuropathic pain, including painful diabetic peripheral
neu-ropathy and postherpetic neuralgia. It is the first drug in the USA approved
for fibromyalgia. In Europe it is approved for general-ized anxiety disorder.
Pharmacokinetics
Gabapentin
is not metabolized and does not induce hepatic enzymes. Absorption is nonlinear
and dose-dependent at very high doses, but the elimination kinetics are linear.
The drug is not bound to plasma proteins. Drug-drug interactions are
negligible. Elimination is via renal mechanisms; the drug is excreted
unchanged. The half-life is relatively short, ranging from 5 to 8 hours; the
drug is typically administered two or three times per day.
Pregabalin,
like gabapentin, is not metabolized and is almost entirely excreted unchanged
in the urine. It is not bound to plasma proteins and has virtually no drug-drug
interactions, again resembling the characteristics of gabapentin. Likewise,
other drugs do not affect the pharmacokinetics of pregabalin. The half-life of
pregabalin ranges from about 4.5 hours to 7.0 hours, thus requir-ing more than
once-daily dosing in most patients.
Related Topics