Chapter: Medical Surgical Nursing: Management of Patients With Female Reproductive Disorders
Pelvic Organ Prolapse: Cystocele, Rectocele, Enterocele
PELVIC
ORGAN PROLAPSE: CYSTOCELE, RECTOCELE, ENTEROCELE
Time
and gravity can put strain on the ligaments and structures that make up the
female pelvis. Childbirth can result in tears of the levator sling musculature,
resulting in structural weakness. Hormone deficiency also may play a role.
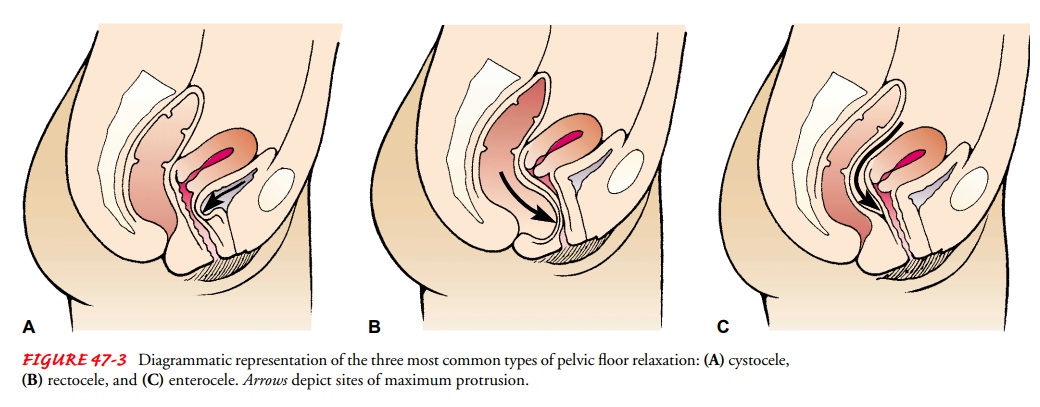
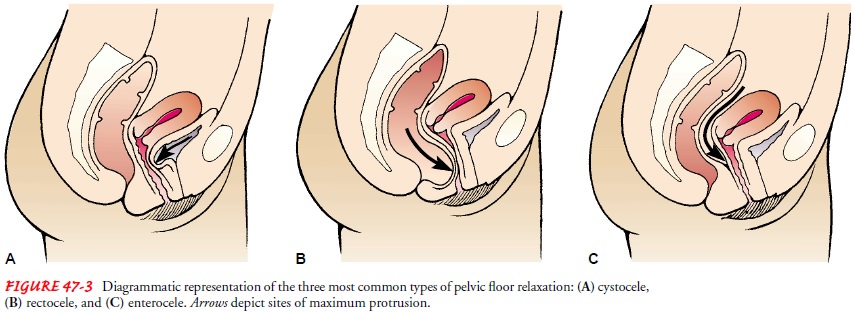
Cystocele is a downward displacement of the bladder towardthe vaginal orifice (Fig. 47-3) resulting from damage to the anterior vaginal support structures.
It usually results from injury and strain during
childbirth. The condition usually appears some years later when genital atrophy
associated with aging occurs, but younger, multiparous, premenopausal women may
also be affected.
Rectocele
and perineal lacerations may affect the muscles and tissues of the pelvic floor
and may occur during childbirth. Be-cause of muscle tears below the vagina, the
rectum may pouch upward, thereby pushing the posterior wall of the vagina
forward. This structural abnormality is called a rectocele. Sometimes the lacerations may completely sever the
fibers of the anal sphincter (complete tear). An enterocele is a protrusion of
the intestinal wall into the vagina. Prolapse (if complete prolapse occurs, it
may also be referred to as procidentia) results from a weakening of the support
structures of the uterus itself; the cervix drops and may protrude from the
vagina.
Clinical Manifestations
Because
a cystocele causes the anterior vaginal wall to bulge downward, the patient may
report a sense of pelvic pressure, fa-tigue, and urinary problems such as
incontinence, frequency, and urgency. Back pain and pelvic pain may occur as
well. The symp-toms of rectocele resemble those of cystocele, with one
exception: instead of urinary symptoms, the patient may experience rectal
pressure. Constipation, uncontrollable gas, and fecal incontinence may occur in
patients with complete tears. Prolapse can result in feelings of pressure and
ulcerations and bleeding. Dyspareunia may occur with these disorders.
Medical Management
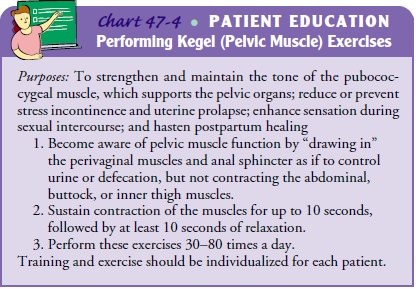
Kegel
exercises, which involve contracting or tightening the vaginal muscles, are
prescribed to help strengthen these weakened muscles. The exercises are more
effective in the early stages of a cystocele. Kegel exercises are easy to do
and are recommended for all women, including those with strong pelvic floor
muscles (Chart 47-4).
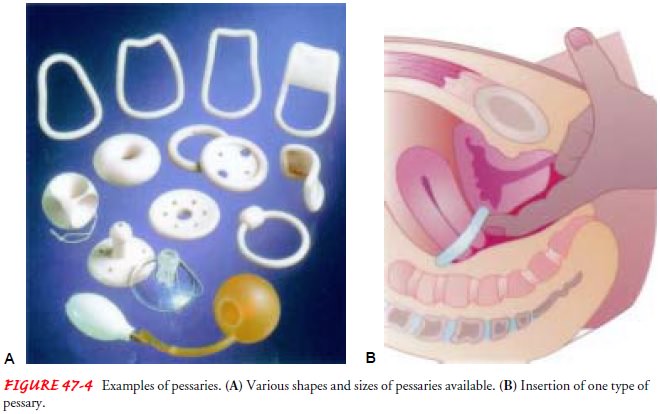
Pessaries
can be used to avoid surgery. This device is inserted into the vagina and
positioned to keep an organ, such as the bladder, uterus, or intestine,
properly aligned when a cystocele, rectocele, or prolapse has occurred.
Pessaries are usually ring-shaped or doughnut-shaped and are made of various
materials, such as rubber or plastic (Fig. 47-4). Rubber pessaries must be
avoided in women with latex allergy. The size and type of pessary are selected
and fitted by a gynecologic health care provider. The patient should have the
pessary removed, examined, and cleaned by her health care provider at
prescribed intervals. At this checkup, vaginal walls are examined for pressure points
or signs of irritation. Normally, the patient experiences no pain, discom-fort,
or discharge with a pessary, but if chronic irritation occurs, alternative
measures may be needed.
SURGICAL MANAGEMENT
In
many cases, surgery helps to correct structural abnormalities. The procedure to
repair the anterior vaginal wall is called anterior colporrhaphy, repair of a rectocele is called a posterior
colporrha-phy, and repair of perineal lacerations is called a perineorrhaphy. These repairs are
frequently performed laparoscopically, resulting in short hospital stays and
good outcomes. A laparoscope is
in-serted through a small abdominal incision, the pelvis is visualized, and
surgical repairs are performed.
Related Topics