Chapter: Medical Surgical Nursing: Management of Patients With Urinary Disorders
Genitourinary Trauma
Genitourinary Trauma
Various
types of injuries of the flank, back, or upper abdomen may result in trauma to
the kidney, ureter, bladder, or urethra. Trauma to the kidney accounts for
about half of all cases of gen-itourinary trauma (Dreitlein, Suner &
Basler, 2001).
RENAL TRAUMA
Normally,
the kidneys are protected by the rib cage and muscu-lature of the back
posteriorly and by a cushion of abdominal wall and viscera anteriorly. They are
highly mobile and are fixed only at the renal pedicle (stem of renal blood
vessels and the ureter). With traumatic injury, the kidney can be thrust
against the lower ribs, resulting in contusion and rupture. Rib fractures or
fractures of the transverse process of the upper lumbar vertebrae may be
as-sociated with renal contusion or laceration. Injuries may be blunt
(automobile and motorcycle crashes, falls, athletic injuries, as-saults) or
penetrating (gunshot wounds, stabbings). Failure to wear seat belts contributes
to the incidence of renal trauma in motor vehicle crashes. Up to 80% of
patients with renal trauma have associated injuries of other internal organs.
Renal
trauma may be classified by the mechanism of injury: blunt or penetrating.
Blunt renal trauma accounts for 80% to 90% of all renal injuries; penetrating
renal trauma accounts for the remaining 10% to 20% (Bayerstock, Simons &
McLoughlin, 2001). Blunt renal trauma is classified into one of four groups, as
follows:
· Contusion: bruises or
hemorrhages under the renal capsule; capsule and collecting system intact
· Minor laceration:
superficial disruption of the cortex; renal medulla and collecting system are
not involved
· Major laceration:
parenchymal disruption extending into cortex and medulla, possibly involving
the collecting system
· Vascular injury: tears
of renal artery or vein
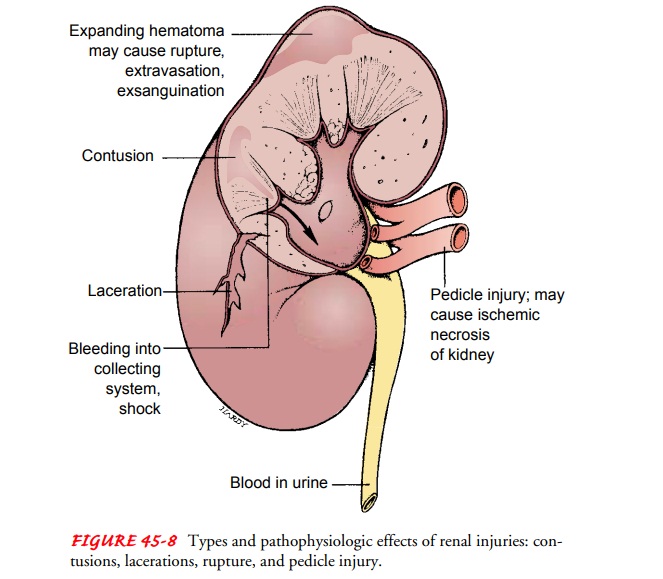
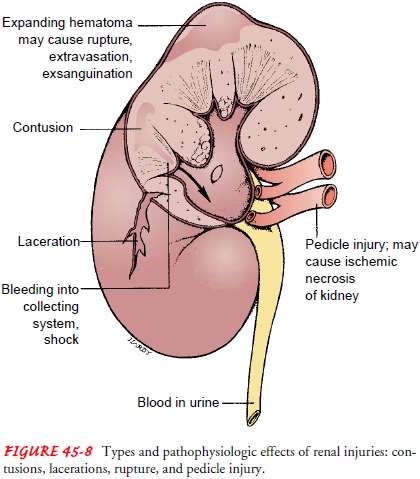
The most common renal injuries are contusions, lacerations, ruptures, and renal pedicle injuries or small internal lacerations of the kidney (Fig. 45-8). The kidneys receive half of the blood flow from the abdominal aorta; therefore, even a fairly small renal laceration can produce massive bleeding. About 70% of patients are in shock when admitted to the hospital (Dreitlein et al., 2001).
Clinical
manifestations include pain, renal colic (due to blood clots or fragments
obstructing the collecting system), hematuria, mass or swelling in the flank,
ecchymoses, and lacerations or wounds of the lateral abdomen and flank.
Hematuria is the most common manifestation of renal trauma; its presence after
trauma suggests renal injury. There is no relationship between the degree of
hematuria and the degree of injury. Hematuria may not occur, or it may be
detectable only on microscopic examination. Signs and symptoms of hypovolemia
and shock are likely with signifi-cant hemorrhage.
URETERAL TRAUMA
Penetrating
trauma and unintentional injury during surgery are the major causes of trauma
to the ureters. Gunshot wounds ac-count for 95% of ureteral injuries, which may
range from contu-sions to complete transection. Unintentional injury to the
ureter may occur during gynecologic or urologic surgery (Mathevet, Valencia,
Cousin et al., 2001; Perez-Brayfield, Keane, Krishnan et al., 2001). There are
no specific signs or symptoms of ureteral injury; many traumatic injuries are
discovered during exploratory surgery. If the ureteral trauma is not detected
and urine leakage continues, fistulas are likely to develop.
Intravenous
urography detects 90% of ureteral injuries and can be performed on the operating
table in patients undergoing emergent surgery. Surgical repair with placement
of stents (to divert urine away from the anastomoses) is usually necessary.
BLADDER TRAUMA
Injury
to the bladder may occur with pelvic fractures and multi-ple trauma or from a
blow to the lower abdomen when the blad-der is full. Blunt trauma may result in
contusion evident as an ecchymosis—a large, discolored bruise resulting from
escape of blood into the tissues and involving a segment of the bladder wall—
or in rupture of the bladder extraperitoneally, intraperitoneally, or both.
Complications from these injuries include hemorrhage, shock, sepsis, and
extravasation of blood into the tissues, which must be treated promptly (Morey,
Iverson, Swan et al., 2001).
URETHRAL TRAUMA
Urethral
injuries usually occur with blunt trauma to the lower abdomen or pelvic region.
Many patients also have associated pelvic fractures. The classic triad of
symptoms comprises blood at the urinary meatus, inability to void, and a
distended bladder ( Jordan, Jezior & Rosenstein, 2001).
Medical Management
The
goals of management in patients with genitourinary trauma are to control
hemorrhage, pain, and infection; to preserve and restore renal function; and to
maintain urinary drainage. In renal trauma, all urine is saved and sent to the
laboratory for analysis to detect RBCs and to evaluate the course of bleeding.
Hemat-ocrit and hemoglobin levels are monitored closely; decreasing val-ues
indicate hemorrhage.
The
patient is monitored for oliguria and signs of hemorrhagic shock because a
pedicle injury or shattered kidney can lead to rapid exsanguination (lethal
blood loss). An expanding hematoma may cause rupture of the kidney capsule. To
detect hematoma, the area around the lower ribs, upper lumbar vertebrae, flank,
and ab-domen is palpated for tenderness. A palpable flank or abdominal mass
with local tenderness, swelling, and ecchymosis suggests renal hemorrhage. The
area of the original mass can be outlined with a marking pencil so that the
examiner can evaluate the area for change.
Renal
trauma is often associated with other injuries to the ab-dominal organs (liver,
colon, small intestines); therefore, the pa-tient is assessed for skin
abrasions, lacerations, and entry and exit wounds of the upper abdomen and
lower thorax because these may be associated with renal injury.
With
renal trauma, such as a contusion of the kidney, heal-ing may take place with
conservative measures. If the patient has microscopic hematuria and a normal
intravenous urogram, out-patient management is possible. If gross hematuria or
a minor laceration is present, the patient is hospitalized and kept on bed rest
until hematuria clears. Antimicrobial medications may be prescribed to prevent
infection from perirenal hematoma or uri-noma (a cyst containing urine).
Patients with retroperitoneal hematomas may develop low-grade fever as
absorption of the clot takes place.
SURGICAL MANAGEMENT
In
renal trauma, any sudden change in the patient’s condition may indicate
hemorrhage and requires surgical intervention.
Depending
on the patient’s condition and the nature of the in-jury, major lacerations may
be treated through surgical interven-tion or conservatively (bed rest, no
surgery). Vascular injuries require immediate exploratory surgery because of
the high inci-dence of involvement of other organ systems and the serious
com-plications that may result if these injuries are untreated. The patient is
often in shock and requires aggressive fluid resuscitation. The damaged kidney
may have to be removed (nephrectomy).
Early
postoperative complications (within 6 months) include rebleeding, perinephritic
abscess formation, sepsis, urine extrava-sation, and fistula formation. Other
complications include stone formation, infection, cysts, vascular aneurysms,
and loss of renal function. Hypertension can be a complication of any renal
surgery but usually is a late complication of renal injury.
In
bladder trauma, treatment for rupture of the bladder in-volves immediate
exploratory surgery and repair of the lacera-tion, suprapubic drainage of the
bladder and the perivesical space (around the bladder), and insertion of an
indwelling uri-nary catheter. In addition to the usual care following urologic
surgery, the drainage systems (suprapubic, indwelling urethral catheter, and
perivesical drains) are closely monitored to ensure adequate drainage until
healing takes place. The patient with a ruptured bladder may have gross
bleeding for several days after repair.
In
urethral trauma, unstable patients who need monitoring of urine output may need
a suprapubic catheter inserted.
The
patient is catheterized after urethrography is performed to minimize the risk
of urethral disruption and extensive, long-term complications, such as
stricture, incontinence, and impotence. Surgical repair may be performed
immediately or at a later time. Delayed surgical repair tends to be the favored
procedure because it is associated with fewer long-term complications, such as
im-potence, strictures, and incontinence. After surgery, an indwelling urinary
catheter may remain in place for up to 1 month.
Nursing Management
The
patient with genitourinary trauma (particularly renal trauma) should be
assessed frequently during the first few days after injury to detect flank and
abdominal pain, muscle spasm, and swelling over the flank.
During
this time, patients can be instructed about care of the incision and the
importance of an adequate fluid intake. In addi-tion, instructions about
changes that should be reported to the physician, such as fever, hematuria,
flank pain, or any signs and symptoms of decreasing kidney function, are
provided. Guide-lines for increasing activity gradually, lifting, and driving
are also provided in accordance with the physician’s prescription.
Follow-up
nursing care includes monitoring the blood pres-sure to detect hypertension and
advising the patient to restrict ac-tivities for about 1 month after trauma to
minimize the incidence of delayed or secondary bleeding. The patient should be
advised to schedule periodic follow-up assessments of renal function
(creatinine clearance, serum BUN and creatinine analyses). If a nephrectomy was
necessary, the patient is advised to wear medical identification.
Related Topics