Chapter: Medical Surgical Nursing: Management of Patients With Urinary Disorders
Acute Glomerulonephritis - Primary Glomerular Diseases
ACUTE
GLOMERULONEPHRITIS
Glomerulonephritis is an inflammation of the glomerular capillaries.
Acute glomerulonephritis is primarily a disease of children older than 2 years
of age, but it can occur at nearly any age.
Pathophysiology
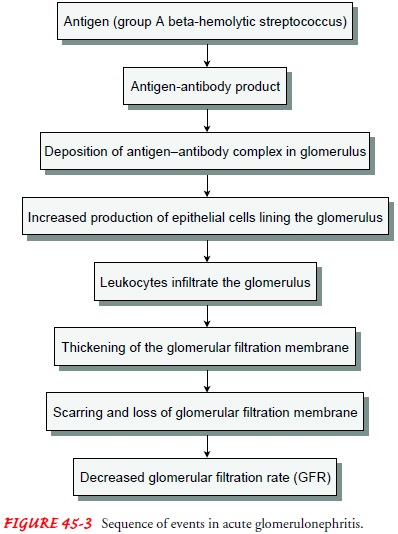
In
most cases of acute glomerulonephritis, a group A beta-hemolytic streptococcal
infection of the throat precedes the onset of glomerulonephritis by 2 to 3
weeks (Fig. 45-3). It may also fol-low impetigo (infection of the skin) and
acute viral infections (upper respiratory tract infections, mumps, varicella
zoster virus, Epstein-Barr virus, hepatitis B, and human immunodeficiency virus
infection). In some patients, antigens outside the body (eg, medications,
foreign serum) initiate the process, resulting in antigen-antibody complexes
being deposited in the glomeruli. In other patients, the kidney tissue itself
serves as the inciting antigen.
Clinical Manifestations
The primary presenting feature of acute glomerulonephritis is hematuria (blood in the urine), which may be microscopic (iden-tifiable through microscopic examination) or macroscopic or gross (visible to the eye). The urine may appear cola-colored because of RBCs and protein plugs or casts. (RBC casts indicate glomerular injury.) Glomerulonephritis may be so mild, however, that hema-turia is discovered incidentally through a routine microscopic uri-nalysis, or the disease may be so severe that the patient has acute renal failure with oliguria. Acute glomerulonephritis typically has an abrupt onset preceded by a latent period between the strepto-coccal infection and the first indications of renal involvement av-eraging 10 days.
Proteinuria
(primarily albumin), which is present, is due to the increased permeability of
the glomerular membrane. BUN and serum creatinine levels may rise as urine
output drops. The patient may be anemic.
Some
degree of edema and hypertension is noted in 75% of patients. In the more
severe form of the disease, the patient also complains of headache, malaise,
and flank pain. Tenderness over the CVA is common. Elderly patients may
experience circulatory overload with dyspnea, engorged neck veins,
cardiomegaly, and pulmonary edema. Atypical symptoms include confusion,
som-nolence, and seizures, which are often confused with the symp-toms of a
primary neurologic disorder.
Assessment and Diagnostic Findings
In
acute glomerulonephritis, the kidneys become large, swollen, and congested. All
renal tissues—glomeruli, tubules, and blood vessels—are affected to varying
degrees. Electron microscopy and immunofluorescent analysis help identify the
nature of the lesion; however, a kidney biopsy may be needed for definitive
diagnosis.
Serial
determinations of antistreptolysin O or anti-DNase B titers are usually
elevated in poststreptococcal glomerulonephritis. Serum complement levels may
be decreased but generally return to normal within 2 to 8 weeks. More than half
of patients with IgA nephropathy (the most common type of primary
glomeru-lonephritis) have an elevated serum IgA and a normal comple-ment level.
If the
patient improves, the amount of urine increases and the urinary protein and
sediment diminish. Usually, more than 90% of children recover. The percentage
of adults who recover is not well established but is probably about 70%. Some
patients be-come severely uremic within weeks and require dialysis for sur-vival.
Others, after a period of apparent recovery, insidiously develop chronic
glomerulonephritis.
Complications
Complications
of acute glomerulonephritis include hypertensive encephalopathy, heart failure,
and pulmonary edema. Hyperten-sive encephalopathy is considered a medical
emergency, and ther-apy is directed toward reducing the blood pressure without
impairing renal function (Tonelli et al., 2001). Although rare, optic
neuropathy in uremia is a medical emergency requiring the immediate institution
of dialysis, corticosteroid therapy, and cor-rection of anemia (Winkelmayer et
al., 2001).
Rapidly
progressive glomerulonephritis is a rapid and pro-gressive decline in renal
function. Without treatment, it results in ESRD in a matter of weeks or months.
Signs and symptoms are similar to those of acute glomerulonephritis (hematuria
and proteinuria), but the course of the disease is more severe and rapid.
Crescent-shaped cells accumulate in Bowman’s space, dis-rupting the filtering
surface. Plasma exchange (plasmapheresis) and treatment with high-dose
corticosteroids and cytotoxic agents have been used to reduce the inflammatory
response. Dialysis is initiated in acute glomerulonephritis if signs and
symptoms of uremia are severe. With aggressive treatment, the prognosis for
patients with rapidly progressive glomerulonephritis is greatly improved.
Medical Management
Management
consists primarily of treating symptoms, attempt-ing to preserve kidney
function, and treating complications promptly. Pharmacologic therapy depends on
the cause of acute glomerulonephritis. If residual streptococcal infection is
sus-pected, penicillin is the agent of choice; however, other antibiotic agents
may be prescribed. Corticosteroids and immunosup-pressant medications may be
prescribed for patients with rapidly progressive acute glomerulonephritis, but
in most cases of post-streptococcal acute glomerulonephritis, these medications
are of no value and may actually worsen the fluid retention and hypertension.
Dietary
protein is restricted when renal insufficiency and ni-trogen retention
(elevated BUN) develop. Sodium is restricted when the patient has hypertension,
edema, and heart failure. Loop diuretic medications and antihypertensive agents
may be prescribed to control hypertension. Prolonged bed rest has little value
and does not alter long-term outcomes.
Nursing Management
Although
most patients with acute uncomplicated glomeru-lonephritis are treated as
outpatients, nursing care is important no matter what the setting. In a
hospital setting, carbohydrates are given liberally to provide energy and
reduce the catabolism of protein. Intake and output are carefully measured and
recorded. Fluids are given according to the patient’s fluid losses and daily
body weight. Insensible fluid loss through the respiratory and GI tracts (500
to 1,000 mL) is considered when estimating fluid loss. Diuresis begins about 1
week after the onset of symptoms with a decrease in edema and blood pressure.
Proteinuria and micro-scopic hematuria may persist for many months, and some
pa-tients may go on to develop chronic glomerulonephritis. Other nursing
interventions focus primarily on patient education for safe and effective
self-care at home.
PROMOTING HOME AND COMMUNITY-BASED CARE
Teaching Patients Self-Care.
Patient
education is directed to-ward maintaining kidney function and preventing
complications. Fluid and diet restrictions must be reviewed with the patient to
avoid worsening of edema and hypertension. The patient is in-structed to notify
the physician if symptoms of renal failure occur (eg, fatigue, nausea,
vomiting, diminishing urine output) or at the first sign of any infection.
Information is given verbally and in writing.
Continuing Care.
The
importance of follow-up evaluations ofblood pressure, urinalysis for protein,
and serum BUN and creatinine levels to determine if the disease has progressed
is stressed to the patient. A referral for home care may be indi-cated; a visit
from a home care nurse provides an opportunity for careful assessment of the
patient’s progress and detection of early signs and symptoms of renal
insufficiency. If cortico-steroids, immunosuppressant agents, or antibiotic
medications are prescribed, the home care nurse or nurse in the outpatient
setting uses the opportunity to review the dosage, desired actions, and adverse
effects of medications and the precautions to be followed
Related Topics