Chapter: Psychology: Psychopathology
Eating Disorders
Eating Disorders
Two
different eating disorders are identified by the DSM. The first—anorexia
nervosa— is defined by a refusal to maintain a minimally appropriate body
weight. The second— bulimia nervosa—is
defined by an alternating sequence of “binges” and “purges”—rapidfood intake
followed by maladaptive (and often extreme) attempts to keep from gain-ing
weight.
ANOREXIA NERVOSA
Individuals
with anorexia nervosa are
preoccupied with food and eating and have an intense fear of gaining weight.
This fear is nurtured by a disturbance in how these people perceive their own
bodies—they genuinely believe themselves to be fat, despite the fact that in
many cases they are extremely, even dangerously, thin (Figure 16.32). They
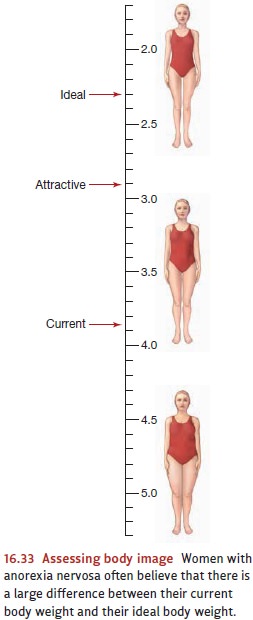
spend enormous amounts of time measuring various parts of their bodies and
critically examining themselves in the mirror. Any slight change in weight is
momentous to them, with tiny decreases celebrated and minute gains lamented
(Figure 16.33). It’s not surprising, therefore, that individuals with anorexia
nervosa relentlessly pursue thinness and usually achieve unhealthy reductions
in body weight through a regimen of incredibly strict dieting. They may also
exercise excessively or purge (self-induce vomiting or misuse laxatives or
diuretics).
The
lifetime prevalence of anorexia nervosa among females is about 0.5%, and
although men can also have anorexia nervosa, they are 10 times less likely than
women to have this disorder. Still, the features associated with anorexia
nervosa are similar for men and for women—including increased risk of
depression and substance abuse. Anorexia nervosa can begin before puberty, but
this is rare. Typically, it develops in adolescence, between the ages of 14 and
18. The prognosis varies considerably. In severe cases, anorexia nervosa can be
life-threatening, as the extreme dieting can lead to dangerous fluid and electrolyte
imbalances. Individuals with less extreme cases often recover fully, although
some continue throughout their lives to show a fluctuating pattern of weight
gain and loss.
Anorexia
nervosa has a clear genetic component (Strober, Freeman, Lampert, Diamond,
& Kaye, 2000), and a person is 10 times as likely to have anorexia ner-vosa
if she has a close relative with the disorder than if she does not.
Sociocultural factors also play a role. Anorexia nervosa is much more common in
cultures that equate being thin with being attractive than in cultures that do
not (Striegel-Moore et al., 2003).
BULIMIA NERVOSA
Like
individuals with anorexia nervosa, individuals with bulimia nervosa are extremely concerned with their weight and
appearance, and this concern fuels disordered eating behavior (Figure 16.34).
Unlike those with anorexia nervosa, however, individuals with bulimia nervosa
often have normal weight (Hsu, 1990). What marks this disorder is the
combination of binge eating and compensatory behavior (Wilson & Pike,
2001). Bingeeating refers to eating
a large amount of food within a relatively brief time period (e.g.,2 hours),
usually while feeling little or no control over what or how much one eats. Compensatory behavior refers to the
actions taken to try to ensure that the binge eat-ing does not translate into
weight gain—including self-induced vomiting, misuse of laxatives or diuretics,
or extreme levels of exercise.
Because
people with bulimia nervosa feel shame about their binges, they often try to
hide their behavior from others and may spend considerable time planning their
secre-tive eating sessions. When they do binge, the targeted foods are
typically high-calorie “junk” foods such as donuts, cake, or ice cream.
Many people binge at one point or another, and some occasionally purge. The DSM diagnosis for bulimia nervosa applies only if a person exhibits binge eating and inappropriate compensatory behaviors at least twice a week for at least 3 months. By this definition, the lifetime prevalence of bulimia nervosa among women is approximately 1 to 3% and—as with anorexia nervosa—it is approximately 10 times more common in women than in men. The onset of bulimia nervosa is usu-ally late adolescence, and over the long term, the ill-ness can lead to many health problems. For example, women whose compensatory behaviors include purging may develop fluid and electrolyte imbalances. The vomiting that is usually associated with bulimia nervosa leads to a significant erosion of dental enamel, giving teeth a worn and yellowed look.
Both
genetic and sociocultural factors contribute to the onset and maintenance of
bulimia nervosa. Women who have close relatives with bulimia nervosa are four
times more likely to have this disorder than are women who do not (Strober et
al., 2000). In addition, research suggests that bulimia nervosa may be confined
to westernized cul-tural contexts (Keel & Klump, 2003); as cultures become
more westernized, rates of bulimia nervosa increase (Nasser, 1997).
Related Topics