Chapter: Case Study in Obstetrics and Gynaecology: Peripartum Care and Obstetric Emergencies
Case Study Reports: Labour
LABOUR
History
A
36-year-old nulliparous woman at term started having uterine tightenings yesterday morning. These were intermittent initially and she managed
to cope with a hot bath and paracetamol, but they have
now become increasingly painful and frequent. This morning she came
in because she
had ruptured membranes at home an hour and
a half ago.
She has continued to notice normal
fetal movements.
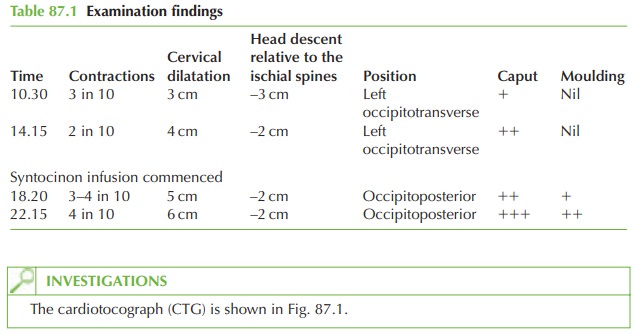
Since arrival the blood pressure, temperature and heart rate have been within the normal range and the liquor has remained clear. She has been examined several times and the findings of each examination are shown in Table 87.1. After the examination at 14.15 a syntocinon infusion was commenced.
Questions
·
How
do you interpret the examination and CTG findings?
·
What factors are associated with this pattern
of labour?
·
How would you manage this woman?
ANSWER
The
examination findings show failure to progress in the first
stage in labour.
Once labour has been
established, the cervix
is expected to dilate at approximately 1 cm/h. In this case, despite attempted augmentation with an oxytocic
(syntocinon), there has only been 3 cm dilatation in almost 12 h.
This situation is most common in nulliparous women and is termed primary
dysfunctional labour. Other associations are malposition (commonly the
occipitoposterior position) and increased fetal size (cephalopelvic disproportion).
Management
Maximum contractions have been achieved (4 in 10 min) with the oxytocic for several
hours, and there are increasing signs of obstruction (caput and moulding
of the fetal head). In view of this the only management option
available is to perform an emergency
Caesarean section.
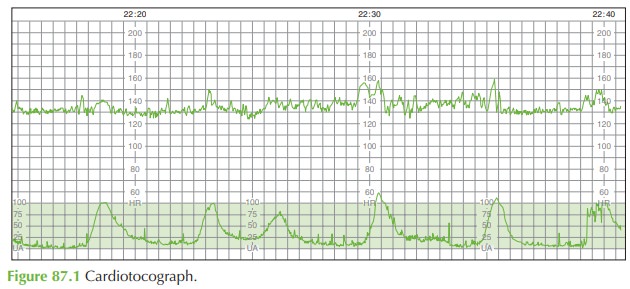
The
CTG is normal,
but without intervention, the likely scenario is for fetal
compromise to occur. Therefore once the decision has been made
to proceed with
Caesarean section, oxy- tocin should be discontinued to reduce the effect of the prolonged contractions on the baby. Delivery
should be arranged
within 30 min of the decision being
made.
The
important points in arranging delivery
by emergency Caesarean section in this case are:
·
informed consent, after appropriate explanation, by the mother
·
informing the anaesthetist and assistant
·
informing the theatre staff and paediatrician
·
ranitidine and metoclopramide to the mother
(usually intravenous) to minimize gastric aspiration should general anaesthetic be needed
·
insertion of an indwelling urinary catheter
·
transfer of the woman to theatre,
with continuous CTG until delivery.

Related Topics