Chapter: Case Study in Obstetrics and Gynaecology: Peripartum Care and Obstetric Emergencies
Case Study Reports: Labour
LABOUR
History
A
31-year-old woman is admitted with contractions at 40 weeks’
gestation. This is her
fourth pregnancy, having
had two terminations approximately 10 years ago and an elect-
ive Caesarean section for breech presentation 3 years ago.
During this pregnancy she has
had an amniocentesis because of a high estimated risk for
Down’s syndrome
at 11–14-week scan.
However a normal
karyotype was
found and subse- quent fetal echocardiography was
normal. In view of her
previous Caesarean section she
was seen by the obstetric consultant in the antenatal clinic at 28 weeks to discuss
mode of deliv- ery. After counselling, a plan was agreed for a vaginal delivery.
She
was admitted with
spontaneous rupture of membranes after
which she had
begun to contract irregularly. The
contractions became stronger and more regular
over the next
2 h after admission
and she requested an epidural.
Vaginal examination was performed
and the cervix was found
to be 4cm dilated. The head was in the occipito transverse position, 1 cm above
the level of the ischial
spines. There was a small
amount of caput
and moulding.
An
epidural was sited
and an indwelling urinary catheter inserted. Three hours later
the woman reported more
severe pain which
did not disappear between contractions. At that
time approximately 200mL
of fresh blood
was seen coming
from the vagina.
Examination
The heart rate is 105/min and blood pressure 105/58 mmHg. The woman feels warm and well
perfused. The abdomen
is soft and the uterus is also soft but very tender, with easy palpation
of fetal parts. On vaginal examination the cervix is 6 cm dilated
and the fetal head feels high in the pelvis and poorly applied to the cervix.
The catheter contains blood-stained urine.
Questions
·
What is the likely diagnosis?
·
How would you manage this patient?
·
What are the possible
further complications in this patient?
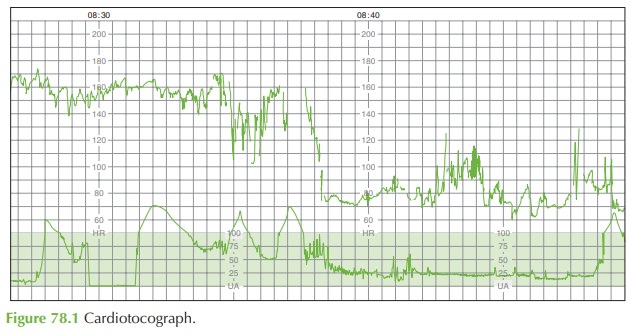
Answer:
The
CTG shows that
the contractions have
stopped. This can
be due to the pressure trans- ducer losing contact
with the patient, but in this
case the combination of other factors
and the fact that
the uterus is soft on palpation suggests that the contractions really have sud- denly stopped.
The
diagnosis is of uterine rupture.
The constant pain, vaginal bleeding,
sudden loss of contractions, change in CTG, easy palpation of fetal parts
and haematuria are all classic features. Uterine rupture is thought to occur in up to 1 in 200 labours
following Caesarean section. It is more common when labour is induced with prostaglandins or augmented
with oxytocin infusion, but may occur
even in an apparently ‘normal’ labour such as this.
Uterine rupture may very rarely occur in women without previous Caesarean section, either because of previous
surgery such as myomectomy, with trauma, or spontaneously.
The major risk factor for
uterine rupture is previous Caesarean section.
General resuscitation measures
should be commenced immediately:
·
large-bore intravenous access
·
full blood count, coagulation test
·
6 unit crossmatch requested
·
intravenous fluids.
The
emergency theatre team,
senior obstetrician and
paediatrician should be summoned
and the woman transferred to theatre immediately for laparotomy, which
may need to be
under general anaesthetic as the epidural is unlikely to be adequate
for laparotomy within a few minutes.
At
laparotomy, the fetus
should be delivered from the abdomen
and the placenta removed. It may be possible to repair the uterine defect.
However, if bleeding
is substantial then other measures may need to be employed such as a B-Lynch haemostatic suture or even hysterectomy.
If the uterus is preserved, then any future pregnancies should be very closely monitored with elective delivery by Caesarean section at 37 weeks’ gestation.
Related Topics