Chapter: Case Study in Obstetrics and Gynaecology: Peripartum Care and Obstetric Emergencies
Case Study Reports: Blood Pressure and Pregnancy
BLOOD PRESSURE AND PREGNANCY
History
A woman
was admitted from the antenatal clinic two
days ago at 38 weeks’
gestation. She is 42 years old
and this is her second
pregnancy. Her
first child was
born by spontaneous vaginal delivery
13 years ago. She has subsequently remarried. Her booking blood
pressure was 138/70 mmHg at 13 weeks.
Her booking blood
tests were unremarkable. At her 36 week
midwife appointment 2 weeks ago,
her blood pressure was 140/85 mmHg
and the urin- alysis was normal. The blood pressure
was repeated 2 days later
and was 140/82
mmHg. Two days ago she saw her midwife
for a further appointment and her blood
pressure was 148/101 mmHg.
Urinalysis showed protein
+.
She feels well in herself
except for swollen
legs. She denies any headache
or blurring of vision.
Examination
She has oedema
to the mid calves and her fingers
are swollen such that she cannot remove her rings. Abdominal palpation is non-tender and
the symphysiofundal height
is 39 cm. Reflexes are normal.
Questions
·
How would you interpret the investigations?
·
What further investigations are needed and how should
she be managed?
ANSWER
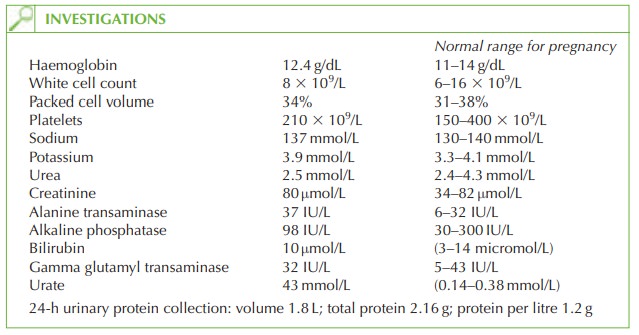
Results interpretation
The haemoglobin and packed cell volume suggest
mild haemoconcentration. The platelet
count is normal for pregnancy, though low for a non-pregnant person. Electrolytes are within the normal range
but the creatinine is higher than normal for pregnancy. Alkaline phosphatase is always raised
in pregnancy due to its production by the placenta. However the alanine transaminase is abnormal.
A normal urate
value correlates with gestational age (the urate
level should not be more than the number of weeks gestation) and therefore the level of 43 mmol/L
is high. Finally, the 24-h urinary protein
measurement, performed to quantify the
degree of proteinuria, has shown a significantly
raised result.
This woman thus has pregnancy-induced hypertension (PIH) with proteinuria, abnormal liver function and raised
serum creatinine and
urate. This is known as pre-eclampsia. The condition commonly occurs in asymptomatic women
and the severity
of symptoms often does not correlate with the disease severity.
No further maternal investigations are needed
but fetal wellbeing needs to be assessed by cardiotocograph and ultrasound assessment for fetal growth
and liquor volume
in view of the
association between pre-eclampsia and intrauterine growth
restriction.
Induction of labour
as soon as possible is indicated, as the fetus
is beyond 37 weeks and delay might increase the likelihood of fulminating pre-eclampsia in the mother
or fetal compromise, including placental abruption. There
is no indication for Caesarean section unless induction is unsuccessful or fetal compromise occurs before or during labour.
Close monitoring of blood
pressure is imperative during and after
labour, as many eclamptic fits occur postnatally.
In this case the woman
agreed to induction of labour and started contracting after the first dose of intravaginal prostaglandin gel. The labour progressed rapidly
with subsequent normal delivery. However the blood
pressure increased in labour to 155/110
mmHg. An epidural was sited to help reduce
the blood pressure. Blood pressure increased further and a
hydralazine infusion was required.
She remained in hospital for 5 days postpartum for blood pressure monitoring, during which time her blood results returned to normal. Postnatally she was converted to oral labetalol for 6 weeks, after which blood pressure was normal, and treatment discontinued.

Related Topics