Chapter: Case Study in Obstetrics and Gynaecology: Peripartum Care and Obstetric Emergencies
Case Study Reports: Labour
LABOUR
History
A
22-year-old woman in her second
pregnancy has arrived
on the labour ward at 38
weeks 3 days. She had a normal
delivery 18 months
ago. This pregnancy has been com- plicated by persistent vomiting
until 20 weeks,
and more recently
by anaemia. She reports
contractions commencing approximately 4 h ago.
She took paracetamol at home and
tried to relieve the
pain with a bath, but
now feels she
cannot cope with
the pain.
She
had a show 2 days
ago but has
had no bleeding since then and
has not noticed
any vaginal leak. She has felt the baby moving normally
all day.
Examination
The
blood pressure is 110/58 mmHg and heart rate is 98/min.
The presentation is cephalic
with 2/5 palpable abdominally. Uterine
contractions are palpable
and the uterus
is non- irritable. On vaginal examination the cervix is 5 cm dilated and
the head is 1 cm above the ischial spines. The fetus is right occipitotransverse with mild caput and moulding.
The membranes are intact
but rupture spontaneously during examination, with
clear liquor draining.
The
woman requests an epidural for
pain relief and
is therefore commenced on continu- ous cardiotocograph monitoring. After 20 min you are called in to review the situation.
Questions
·
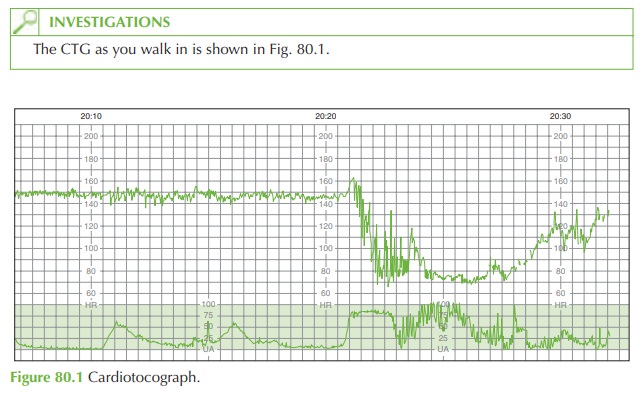
Describe the CTG.
·
What are the possible
causes of this CTG?
·
What management would be appropriate now?
ANSWER
CTG interpretation
The
initial 15 min of CTG shows a baseline of 145/min with normal variability (12/min) and no visible
acceleration or decelerations. Following this there is a drop in fetal heart rate to 70/min for 7 min before gradual
recovery to 125/min.
Contractions are 2 in 10 until the tocograph becomes unreadable.
This is a previously low-risk pregnancy and this CTG shows a fetal bradycardia (reduction in baseline heart rate to below 100/min). In many cases no cause is identified.
Management
If
a bradycardia continues
for more than 5 min, plans should be made to deliver
imme- diately by ‘crash’
Caesarean section under
general anaesthetic. The labour ward theatre
team should be called (including anaesthetist, obstetric registrar, paediatrician, midwife in charge, theatre staff) and the woman
transferred to the operating theatre.
On occasion the bradycardia recovers as preparation is underway for the Caesarean, in which case the plan may
be reviewed. Otherwise the baby should
be delivered immediately.
In
this case the bradycardia did not recover
and the baby was delivered within 12 min of
the decision being made. No cause was
found for the
bradycardia at Caesarean section.
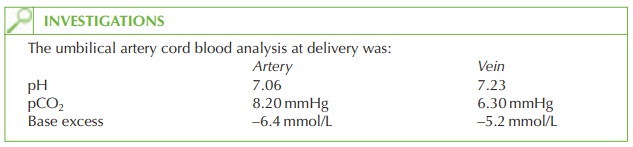
The
baby initially made poor respiratory effort and had a heart
rate less than 100/min, but recovered quickly with drying
and warming. The Apgar score
for the baby was 5 at 1 min
and 9 at 5 min.

Related Topics