Chapter: Clinical Anesthesiology: Anesthetic Management: Anesthesia for Patients with Cardiovascular Disease
Anticoagulation
ANTICOAGULATION
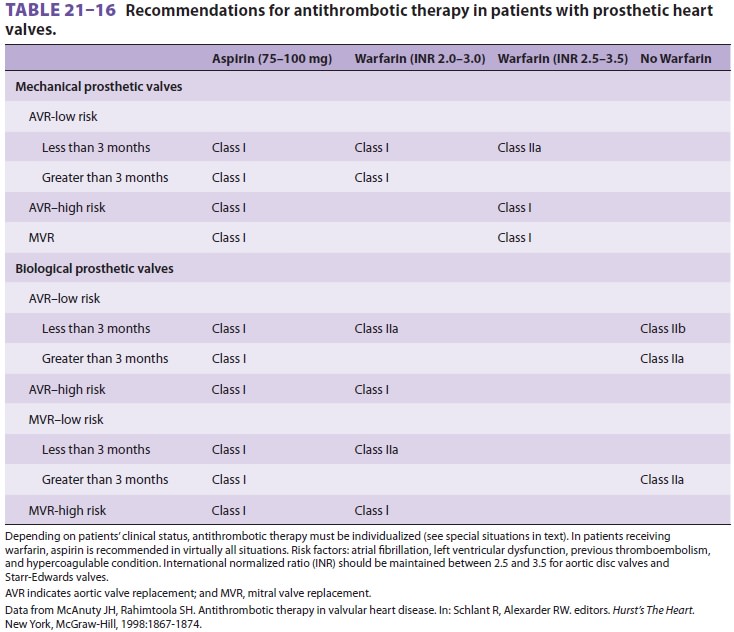
Patients with mechanical prosthetic
heart valves require anticoagulation, which is currently accom-plished with
warfarin. Aspirin is also indicated in this population, as well as in patients
with bio-prosthetic valves, to prevent thrombus formation. Warfarin is
sometimes also used initially for mitral bioprosthetic valves ( Table 21–16).
Patients with prosthetic valves often
present for noncardiac surgery that will require temporary discontinuation of
anticoagulation. The ACC/AHA guidelines indicate that patients at low risk of
throm-bosis, such as those with bileaflet mechanical valves
in the aortic position with no additional
problems (eg, no AF or no hypercoaguable state) can discon-tinue warfarin 48–72
hours preoperatively so that the INR falls below 1.5. In patients at greater
risk of thrombosis, warfarin should be discontinued and heparin, either
unfractionated or low molecular weight, started when the INR falls below 2.0.
Heparin can be discontinued 4–6 hours prior to surgery and then restarted as
soon as surgical bleeding permits, until the patient can be restarted on
warfarin therapy. Fresh frozen plasma may be given, if needed, in an emergency
situation to interrupt warfarin therapy. Vitamin K should not be administered,
as it could potentially lead to a hypercoaguable state. Anesthesia staff should
always consult with the patient’s surgeon and the physician responsible for
prescribing the anticoagulation before adjusting anticoagulation or
antiplatelet regimens perioperatively.
Related Topics