Chapter: Basic & Clinical Pharmacology : Antiprotozoal Drugs
Treatment of Specific Forms of Amebiasis
AMEBIASIS
Amebiasis is infection
with Entamoeba histolytica. This
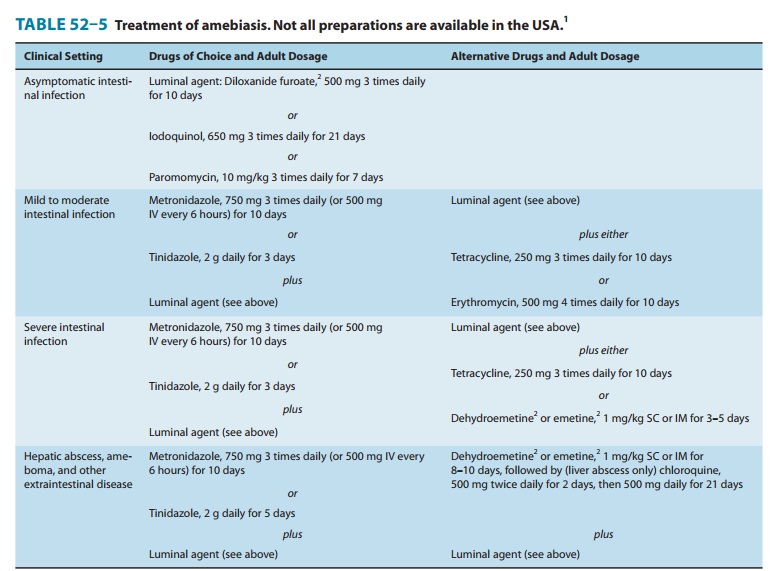
organism can cause asymptomatic intestinal infection, mild to moderate colitis,
severe intestinal infection (dysentery), ameboma, liver abscess, and other
extraintestinal infections. The choice of drugs for amebiasis depends on the
clinical presentation (Table 52–5).
Treatment of Specific Forms of Amebiasis
A. Asymptomatic Intestinal Infection
Asymptomatic carriers
generally are not treated in endemic areas, but in nonendemic areas they are
treated with a luminal amebi-cide. A tissue amebicidal drug is unnecessary.
Standard luminal amebicides are diloxanide furoate, iodoquinol, and
paromomycin. Each drug eradicates carriage in about 80–90% of patients with a
single course of treatment. Therapy with a luminal amebicide is also required
in the treatment of all other forms of amebiasis.
B. Amebic Colitis
Metronidazole plus a
luminal amebicide is the treatment of choice for amebic colitis and dysentery.
Tetracyclines and erythromycin are alternative drugs for moderate colitis but
are not effective against extraintestinal disease. Dehydroemetine or emetine
can also be used, but are best avoided because of toxicity.
C. Extraintestinal Infections
The treatment of
choice for extraintestinal infections is metron-idazole plus a luminal
amebicide. A 10-day course of metronida-zole cures over 95% of uncomplicated
liver abscesses. For unusual cases in which initial therapy with metronidazole
has failed, aspi-ration of the abscess and the addition of chloroquine to a
repeat course of metronidazole should be considered. Dehydroemetine and emetine
are toxic alternative drugs.
Related Topics