Chapter: Basic & Clinical Pharmacology : Antiprotozoal Drugs
Chemoprophylaxis & Treatment - Malaria
CHEMOPROPHYLAXIS & TREATMENT
When patients are
counseled on the prevention of malaria, it is imperative to emphasize measures
to prevent mosquito bites (eg, with insect repellents, insecticides, and bed
nets), because parasites are increasingly resistant to multiple drugs and no
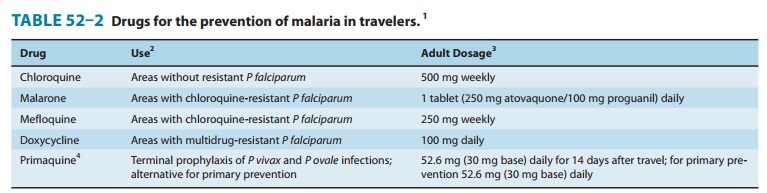
chemoprophy-lactic regimen is fully protective. Current recommendations from
the Centers for Disease Control and Prevention (CDC) include the use of
chloroquine for chemoprophylaxis in the few areas infested by only
chloroquine-sensitive malaria parasites (princi-pally the Caribbean and Central
America west of the Panama Canal), mefloquine or Malarone∗ for most other malarious areas, and
doxycycline for areas with a very high prevalence of multidrug-resistant
falciparum malaria (principally border areas of Thailand) (Table 52–2). CDC
recommendations should be checked regularly (Phone: 770-488-7788; Internet: http://www.cdc.gov/malaria), because these may
change in response to changing resistance patterns and increasing experience
with new drugs. In some circumstances, it may be appropriate for travelers to
carry supplies of drugs with them in case they develop a febrile illness when
medical attention is unavailable. Regimens for self-treatment include new
artemisinin-based combination therapies ,which are widely available
internationally (and, in the case of Coartem∗∗, in the USA); Malarone; mefloquine; and
quinine. Most authorities do not recommend routine terminal chemopro-phylaxis
with primaquine to eradicate dormant hepatic stages of P vivax and P ovale after
travel, but this may be appropriate insome circumstances, especially for
travelers with major exposure to these parasites.
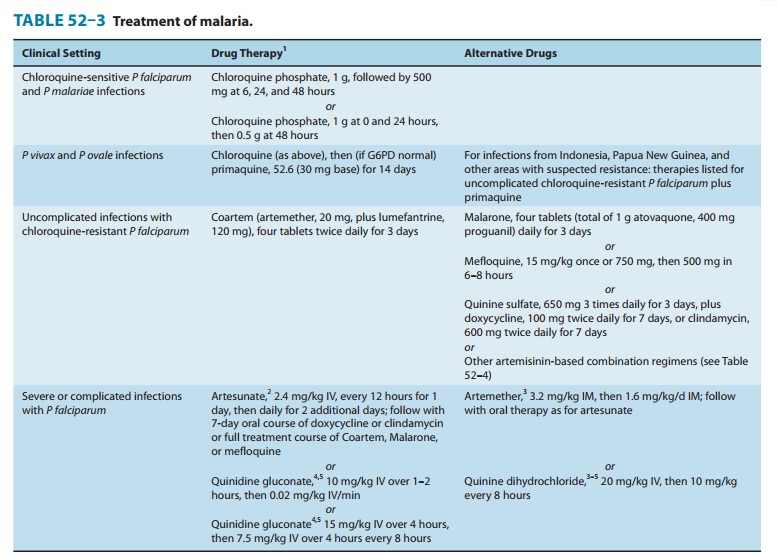
Multiple drugs are
available for the treatment of malaria that presents in the USA (Table 52–3).
Most nonfalciparum infections and falciparum malaria from areas without known
resistance should be treated with chloroquine. For vivax malaria from areas
with suspected chloroquine resistance, including Indonesia and Papua New
Guinea, other therapies effective against falciparum malaria may be used. Vivax
and ovale malaria should subsequently be treated with primaquine to eradicate
liver forms. Uncomplicated falciparum malaria from most areas is typically
treated with Malarone or oral quinine, but new artemisinin-based combina-tions
are increasingly the international standard of care, and one combination,
Coartem, is now available in the USA. Other agents that are generally effective
against resistant falciparum malaria include mefloquine and halofantrine, both
of which have toxicity concerns at treatment dosages. Severe falciparum malaria
is treated with intravenous artesunate, quinidine, or quinine (intravenous
quinine is not available in the USA).
Related Topics