Chapter: Ophthalmology: Retina
Retina
Retina
Basic Knowledge
The retina is the innermost of three successive layers of the globe. It comprises two
parts:
âť– A photoreceptive part (pars optica retinae), comprising the first nine of the 10 layers listed
below.
âť– A nonreceptive part (pars caeca retinae) forming the epithelium of the cil-iary body
and iris.
The pars optica retinae merges with the pars
ceca retinae at the ora serrata.
Embryology:
The retina develops from adiverticulum
of the forebrain(proen-cephalon). Optic vesicles develop which then
invaginate to form a double-walled bowl, the optic cup. The outer wall becomes
the pigment epithelium, and the inner wall later differentiates into the nine
layers of the retina. The retina remains linked to the forebrain throughout
life through a structure known as the retinohypothalamic tract.
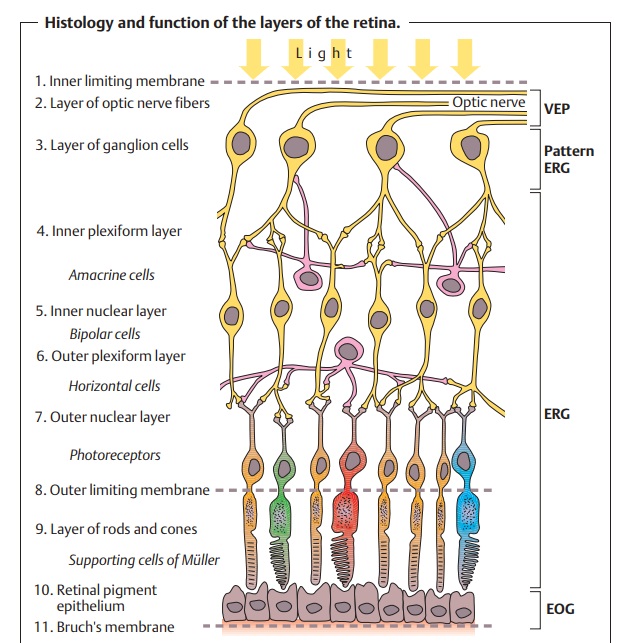
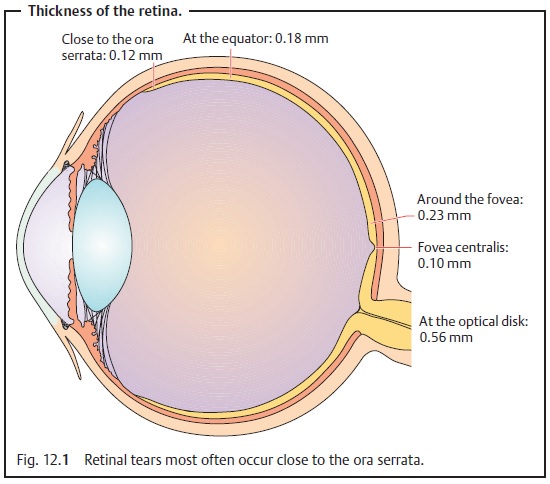
Thickness of the retina (Fig. 12.1)
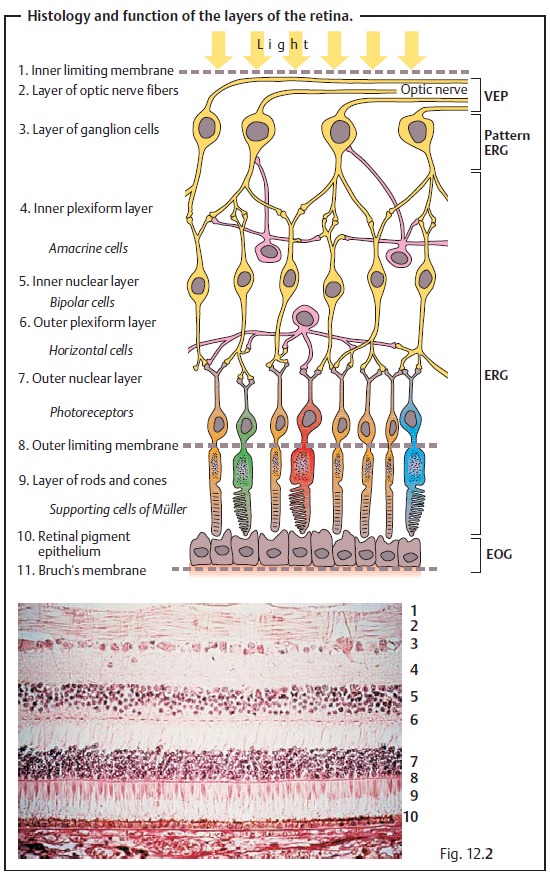
Layers of the retina:
Moving inward along the path of incident light, theindividual
layers of the retina are as follows (Fig. 12.2):
1.
Inner limiting membrane (glial cell fibers separating the retina
from the vitreous body).
2.
Layer of optic nerve fibers (axons of the third neuron).
3.
Layer of ganglion cells (cell nuclei of the multipolar ganglion
cells of the third neuron; “data acquisition system”).
4.
Inner plexiform layer (synapses between the axons of the second
neuron and dendrites of the third neuron).
5.
Inner nuclear layer (cell nuclei of the bipolar nerve cells of
the second neuron, horizontal cells, and amacrine cells).
6.
Outer plexiform layer (synapses between the axons of the first
neuron and dendrites of the second neuron).
7.
Outer nuclear layer (cell nuclei of the rods and cones = first
neuron).
8. Outer limiting membrane (sieve-like plate of processes of glial cells through which rods and cones project).
9.
Layer of rods and cones (the actual photoreceptors).
10.Retinal pigment epithelium (a single cubic layer of heavily
pigmented epithelial cells).
11.
Bruch’s membrane (basal membrane of the choroid separating the
retina from the choroid).
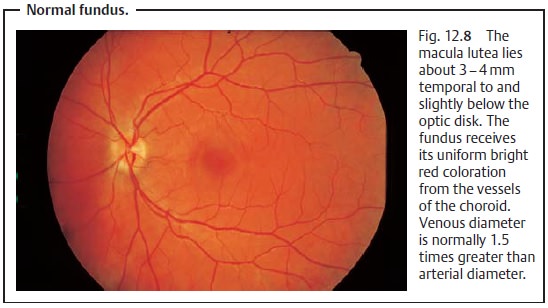
Macula lutea:
The macula lutea is a flattened oval area in the center of theretina approximately 3 – 4 mm (15 degrees) temporal to and slightly below the optic disk. Its diameter is roughly equal to that of the optic disk (1.7 – 2 mm). The macula appears yellow when examined under green light, hence the name macula lutea (yellow spot). Located in its center is the avascular fovea centralis, the point at which visual perception is sharpest.
The fovea centralis contains only cones (no rods) each
with its own neural supply, which explains why this region has such distinct
vision. Light stimuli in this region can directly act on the sensory cells
(first neuron) because the bipolar cells (sec-ond neuron) and ganglion cells
(third neuron) are displaced peripherally.
Vascular supply to the retina:
Theinner layersof the
retina (the inner lim-iting membrane through the inner nuclear layer) are
supplied by the central artery of the retina. This originates at the ophthalmic
artery, enters the eye with the optic nerve, and branches on the inner surface
of the retina. The cen-tral artery is a genuine artery with a diameter of 0.1
mm. It is a terminal artery without anastomoses and divides into four main
branches (see Fig. 12.8).
Because the central artery is a terminal
artery, occlusion will lead to retinal infarction.
The outer layers (outer plexiform layer through the pigment
epithelium) con-tain no capillaries. They are nourished by diffusion primarily
from the richly supplied capillary layer of the choroid. The retinal arteries are normally bright red, have
bright red reflex strips (see Fig. 12.8) that become paler withadvancing age, and do
not show a pulse. The retinal veins are dark red with a
narrow reflex strip, and may show spontaneous pulsation on the optic disk.
Pulsation in the retinal veins is normal;
pulsation in the retinal arteries is abnormal.
The walls of the vessels are transparent so
that only the blood will be visible on ophthalmoscopy. In terms of their
structure and size, the retinal vessels are arterioles and venules, although
they are referred to as arteries and veins. Venous diameter is normally 1.5 times greater than arterial diameter. Capil-laries are
not visible.
Nerve supply to the retina:
The neurosensory retina has no sensory supply. Disorders of the retina are painless because
of the absence of sensory supply.
Light path through the retinal layers:
When electromagnetic radiation inthe visible
light spectrum (wavelengths of 380 – 760 nm) strikes the retina, it is absorbed
by the photopigments of the outer layer. Electric signals are created in a
multi-step photochemical reaction. They reach the photoreceptor synapses as
action potentials where they are relayed to the second neuron. The signals are
relayed to the third and fourth neurons and finally reach the visual cortex.
Light must pass through three layers of cell nuclei before it
reaches the photosensitive rods and cones. This inverted position of the
photore-ceptors is due to the manner in which the retina develops from a
diver-ticulum of the forebrain.
Sensitivity of the retina to light intensity:
The retina has two types of pho-toreceptors,
the rods and the cones. The 110 – 125 million rods permit mesopic and scotopic vision (twilight and night
vision). They are about 500 times more photosensitive than the cones and
contain the photopigment rhodopsin.
Twilight vision decreases after the age of 50,
particularly in patients with additional age-related miosis, cataract, and
decreased visual acu-ity. Therefore, glaucoma patients undergoing treatment
with miotic agents should be advised of the danger of operating motor vehicles
in twilight or at night.
The six to seven million cones in the macula are responsible for photopic vision (daytime vision), resolution, and color perception.
There are threetypes of cones:
âť–blue cones,
âť– green cones,
âť– red cones.
Their photopigments contain the same retinal
but different opsins. Beyond a certain visual field luminance, a transition from dark adaptation to light
adaptation occurs. Luminance refers to the luminous flux per unit solid angle
per unit projected area, measured in candelas per square meter (cd/m2). The cones are responsible for vision up to a luminance of 10
cd/m2, the rods up to 0.01 cd/m2 (twilight vision is 0.01 – 10 cd/m2; night vision is less than 0.01 cd/m2).
Adaptation is the adjustment of the sensitivity of the retina to
varyingdegrees of light intensity. This is done by dilation or contraction of
the pupil and shifting between cone and rod vision. In this manner, the human
eye is able to see in daylight and at night. In light adaptation, the rhodopsin is bleached out so that rod vision
is impaired in favor of cone vision. Light adap-tation occurs far more quickly
than dark adaptation. In dark adaptation,
the rhodopsin quickly regenerates within five minutes (immediate adaptation),
and within 30 minutes to an hour there is a further improvement in night vision
(long-term adaptation). An adaptometer
may be used to determine the light intensity threshold. First the patient is
adapted to bright light for 10 minutes. Then the examining room is darkened and
the light intensity threshold is measured with light test markers. These
measurements can be used to obtain an adaptation curve (Fig. 12.3).

Sensitivity to glare: Glare refers todisturbing brightness within the visual fieldsufficiently greater than the luminance to which the eyes are adapted such asthe headlights of oncoming traffic or intense reflected sunlight. Because the retina is adapted to a lesser luminance, vision is impaired in these cases. Often the glare will cause blinking or elicit an eye closing reflex. Sensitivity to glare can be measured with a special device. Patients are shown a series of visual symbols in rapid succession that they must recognize despite intense glare.
The sensitivity to glare or the speed of
adaptation and readaptation of the eye is important in determining whether the
patient is fit to operate a motor vehicle.
Related Topics