Chapter: Ophthalmology: Retina
Retinal Vein Occlusion
Retinal Vein Occlusion
Definition
Vein occlusion occurs as a result of
circulatory dysfunction in the central vein or one of its branches.
Epidemiology:
Retinal vein occlusion is the second most frequentvascularretinal disorder after diabetic
retinopathy. The most frequent underlying sys-temic disorders are arterial
hypertension and diabetes mellitus; the most frequent underlying ocular
disorder is glaucoma.
Frequent underlying systemic disorders of
retinal vein occlusion include arterial hypertension and diabetes mellitus.
Frequent underlying ocular disorders include glaucoma and retinal vasculitis.
Etiology:
Occlusion of the central vein of the retina or its branches
isfrequently due to local thrombosis at sites where sclerotic arteries compress
the veins. In central retinal vein
occlusion, the thrombus lies at the level of the lamina cribrosa; in branch retinal vein occlusion, it is
frequently at an arteriovenous crossing.
Symptoms:
Patients only notice a loss of visual acuity if the macula or
opticdisk are involved.
Diagnostic considerations and findings:
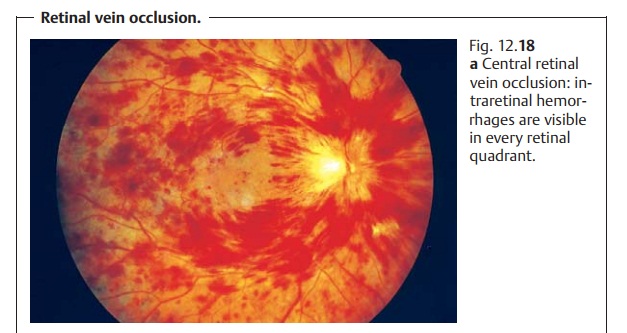
Central retinal vein occlusion canbe diagnosed
where linear or punctiform hemorrhages are seen to occur in all four quadrants
of the retina (Fig. 12.18a). Often
one will find distended and increasingly meandering veins. In branch retinal vein occlusion,
intraretinal hemorrhages will occur in the area of vascular supply; this
bleeding may occur in only one quadrant (Fig. 12.18b) or in two quadrants (hemispheric vein occlusion). Cotton-wool
spots and retinal or optic-disk edema may also be present (simultaneous retinal
and optic-disk edema is also possible). Chronic occlusions may also be
accompanied by lipid deposits. One differen-tiates between non-ischemic and ischemic
occlusion depending on the extent of capillary occlusion. Ischemic occlusion is
diagnosed with the aid of fluorescein angiography.

Differential diagnosis:
Other forms of vascular retinal disease must beexcluded,
especially diabetic retinopathy. An internist should be consulted to verify or
exclude the possible presence of an underlying disorder.
Treatment:
In theacute stage of vein
occlusion,hematocrit should bereduced to 35 – 38% by hemodilution. Laser
treatment is performed in ischemic occlusion that progresses to
neovascularization or rubeosis iridis. Focal laser treatment is performed in branch retinal vein occlusion withmacular
edema when visual acuity is reduced to 20/40 or less within threemonths of
occlusion.
Prophylaxis:
Early diagnosis and prompt treatment of underlying systemicand
ocular disorders is important.
Clinical course and prognosis:
Visual acuity improves in approximately one-third of all
patients, remains unchanged in one-third, and worsens in one-third despite
therapy. Complications include preretinal neovascularization, retinal
detachment, and rubeosis iridis with angle closure glaucoma.
Related Topics