Chapter: Ophthalmology: Vitreous Body
Surgical Treatment: Vitrectomy
Surgical Treatment: Vitrectomy
Definition
Surgical removal and replacement of the
vitreous body with Ringer’s solution, gas, or silicone oil.
Indication:
The primary indications include:
❖ Unabsorbed vitreous hemorrhage.
❖ Tractional retinal detachment.
❖ Proliferative vitreoretinopathy.
❖ Removal of intravitreal displaced lenses or
foreign bodies.
❖Severe postoperative or post-traumatic
inflammatory vitreous changes.
Procedure:
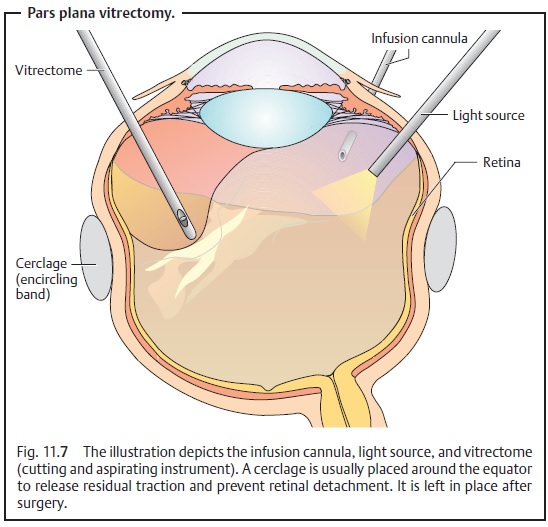
The vitreous body cannot simply be aspirated from the eye as thevitreoretinal attachments would also cause retinal detachment. The pro-cedure requires successive, piecemeal cutting and aspiration with a vitrectome (a specialized cutting and aspirating instrument). Cutting and aspiration of the vitreous body is performed with the aid of simultaneous infusion to pre-vent the globe from collapsing. The surgical site is illuminated by a fiberoptic light source. The three instruments (infusion cannula, light source, and vit-rectome), all 1 mm in diameter, are introduced into the globe through the pars plana, which is why the procedure is referred to as a pars plana vit-rectomy (PPV). This site entails the least risk of iatrogenic retinal detachment(Fig. 11.7). The surgeon holds the vitrectome in one hand and the light source in the other. The procedure is performed under an operating microscope with special contact lenses placed on the corneal surface. Once the vitreous body and any vitreous membranes have been removed (Fig. 11.7), the retina can be treated intraoperatively with a laser (for example, to treat proliferative dia-betic retinopathy or repair a retinal tear). In many cases, such as with an unabsorbed vitreous hemorrhage, it is sufficient to fill the eye with Ringer’s solution following vitrectomy.
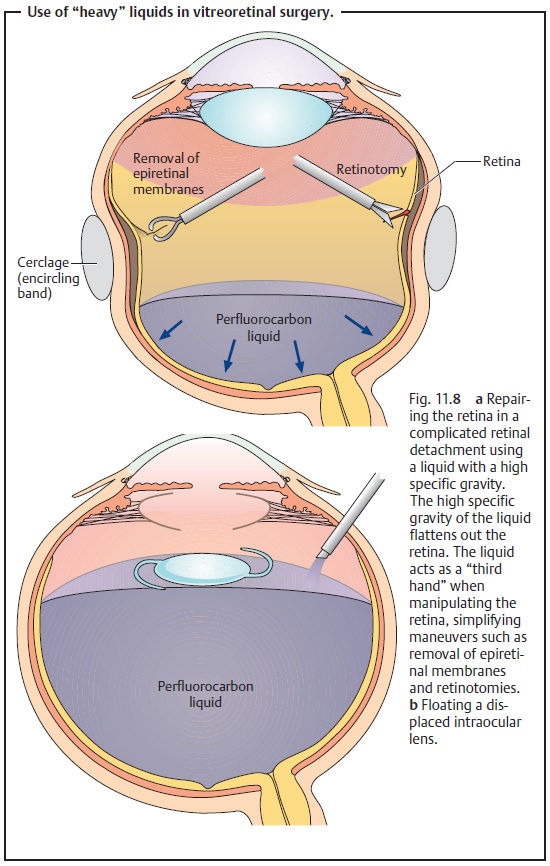
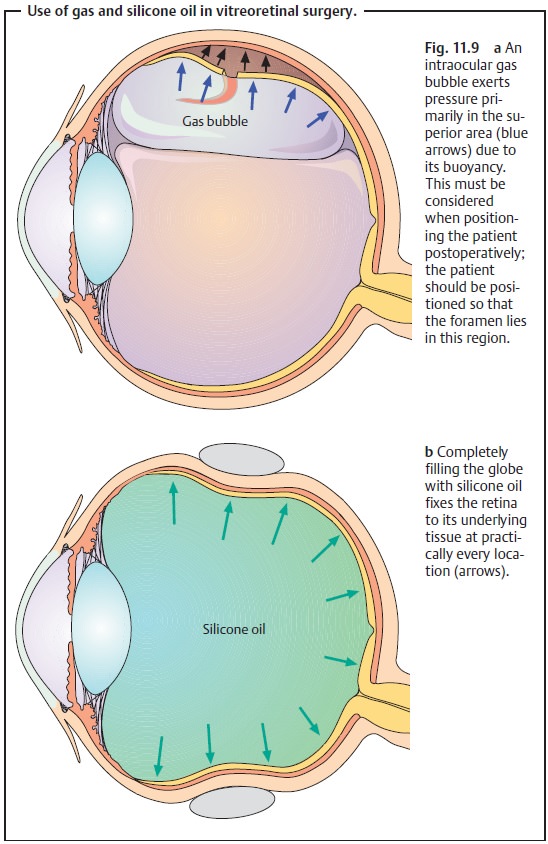
Filling the eye with Ringer’s solution is not sufficient to treat a compli-cated retinal detachment with epiretinal or subretinal membranes and con-traction of the surface of the retina (see proliferative vitreoretinopathy). In these cases, the detached retina must be flattened from anterior to posterior and held with a tamponade of fluid with a very high specific gravity such as a perfluorocarbon liquid (Fig. 11.8a). These “heavy” liquids can also be used to float artifical lenses that have become displaced in the vitreous body. The artificial lenses have a lower specific gravity than these liquids and will float on them (Fig. 11.8b). At the end of the operation, these heavy liquids must be replaced with gases, such as a mixture of air and sulfur hexafluoride, that are spontaneously absorbed within a few days or with silicone oil (which must be removed in a second operation). Postoperative patient positioning should reflect the fact that maximum gas pressure will be in the superior region (Fig. 11.9a) due to its buoyancy. Complicated retinal detachments will require a prolonged internal tamponade. Silicone oil has proven effective for this purpose as it completely fills the vitreous chamber and exerts permanent pres-sure on the entire retina (Fig. 11.9b).
However, silicone oil inevitably causes cataract formation
and occasionally corneal changes and glaucoma. There-fore, it must be removed
in a second operation.
Complications:
Vitrectomy nearly always leads to subsequent
lens opacifica-tion, and rarely to retinal tears, bleeding, or endophthalmitis.
Related Topics