Chapter: Ophthalmology: Vitreous Body
Vitreous Hemorrhage
Vitreous Hemorrhage
Definition
Bleeding into the vitreous chamber or a space created by
vitreous detachment.
Epidemiology:
The annual incidence of this disorder is seven cases per 100000.
Etiology:
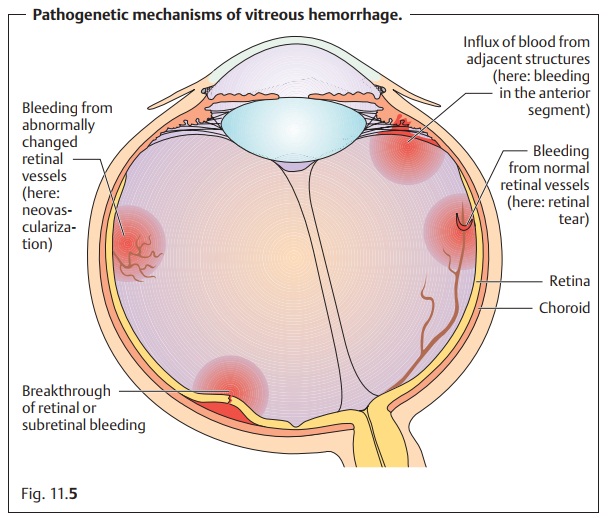
A vitreous hemorrhage may involve one of three possiblepatho-genetic mechanisms (Fig. 11.5):
❖ 1. Bleeding from normal retinal vessels as can occur as a result of mechani-cal
vascular damage in acute vitreous detachment or retinal tear.
❖ 2. Bleeding from retinal vessels with abnormal changes as can occur as a result of
retinal neovascularization in ischemic retinopathy or retinal mac-roaneurysms.
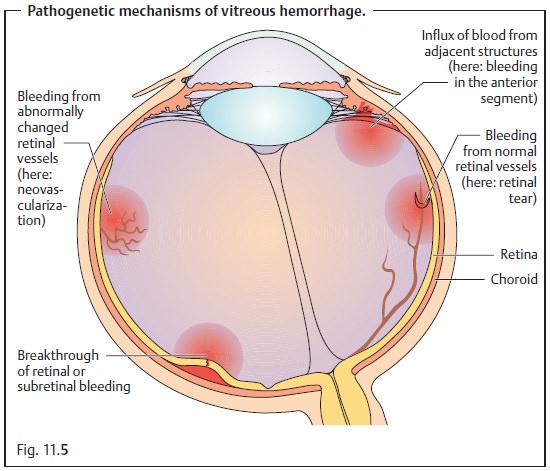
❖ 3.Influx
of blood from the retina or other sources such as the subretinal space or
the anterior segments of the eye.
❖ Posterior vitreous detachment with or without
retinal tears (38%).
❖ Proliferative diabetic retinopathy (32%).
❖ Branch retinal vein occlusion (11%).
❖ Age-related macular degeneration (2%).
❖ Retinal macroaneurysm (2%).
Less frequent causes of vitreous hemorrhage include:
❖
Arteriosclerosis.
❖ Retinal periphlebitis.
❖ Terson’s syndrome (subarachnoid hemorrhage,
increase in intraocular pressure, acutely impaired drainage of blood from the
eye, dilation and rupture of retinal vessels, retinal and vitreous hemorrhage).
❖ Penetrating trauma.
❖ Retinal vascular tumors.
Symptoms:
Patients often report the sudden occurrence of black
opacitiesthat they may describe as “swarms
of black bugs” or “black rain.”
These are dis-tinct from the brighter and less dense floaters seen in synchysis
and vitreous detachment. Severe vitreous hemorrhage can significantly reduce visual acu-ity. Approximately 10µl of blood are sufficient to reduce visual acuity to per-ception
of hand movements in front of the eye.
Diagnostic considerations:
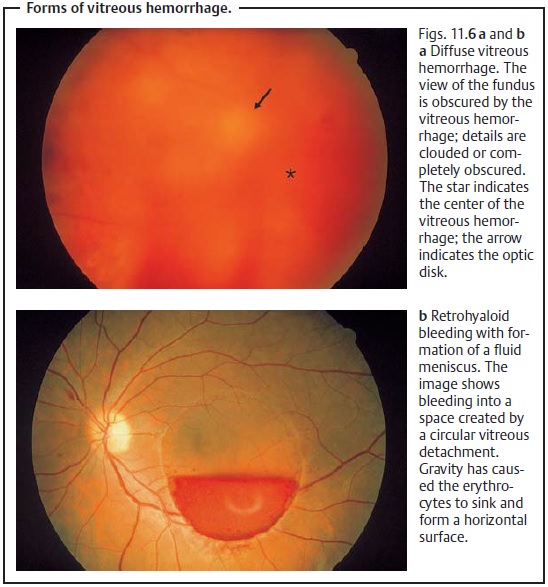
Hemorrhages into the
vitreous body itselfdo notexhibit any characteristic limitations but spread diffusely (the blood cannot form a fluid
meniscus in the gelatinous vitreous
body) and coagulation occurs quickly (Fig. 11.6). Vitreous hemorrhages require examination with an
oph-thalmoscope or contact lens. The contact lens also permits examination of
the retina at a higher resolution so that the examiner is better able to
diagnose small retinal tears than with an ophthalmoscope. Ultrasound studies
are indi-cated where severe bleeding significantly obscures the fundus
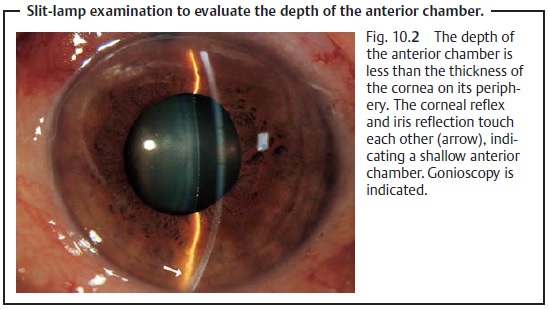
examination. Bleeding in the tissues
adjacent to the vitreous body, i.e., in the retrohyaloidspace, Berger’s
space, or Petit’s space (Fig. 11.2),
can produce a characteristicfluid
meniscus. This meniscus will be visible under slit-lamp examination(Fig.
11.6b).
Treatment:
Patients with acute vitreous hemorrhage should be placed in anupright resting position. This has two
beneficial effects:
❖ 1. The bleeding usually does not continue to
spread into the vitreous body.
❖ 2. The blood in the retrohyaloid space will
settle more quickly.
Next the cause
of the vitreous hemorrhage should be treated, for example a ret-inal tear
may be treated with a laser. Vitrectomy will be required to drain any vitreous
hemorrhage that is not absorbed.
Clinical course and prognosis:
Absorption of a
vitreous hemorrhage is a longprocess. The clinical course will depend on the
location, cause, and severity of the bleeding. Bleeding in the vitreous body
itself is absorbed particularly slowly.
Related Topics