Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Hepatic Disorders
Other Manifestations of Liver Dysfunction
OTHER
MANIFESTATIONS OF LIVER DYSFUNCTION
Edema and Bleeding
Many
patients with liver dysfunction develop generalized edema from hypoalbuminemia
that results from decreased hepatic pro-duction of albumin. The production of
blood clotting factors by the liver is also reduced, leading to an increased
incidence of bruis-ing, epistaxis, bleeding from wounds, and, as described
above, GI bleeding.
Vitamin Deficiency
Decreased
production of several clotting factors may be due, in part, to deficient
absorption of vitamin K from the GI tract. This probably is caused by the
inability of liver cells to use vitamin K to make prothrombin. Absorption of
the other fat-soluble vitamins (vitamins A, D, and E) as well as dietary fats
may also be impaired because of decreased secretion of bile salts into the
intestine.Another group of problems common to patients with severe chronic
liver dysfunction results from inadequate intake of suffi-cient vitamins. Among
the specific deficiency states that occur on this basis are:
•
Vitamin A deficiency, resulting in night blindness
and eye and skin changes
•
Thiamine deficiency, leading to beriberi,
polyneuritis, and Wernicke-Korsakoff psychosis
•
Riboflavin deficiency, resulting in characteristic
skin and mucous membrane lesions
•
Pyridoxine deficiency, resulting in skin and mucous
mem-brane lesions and neurologic changes
•
Vitamin C deficiency, resulting in the hemorrhagic
lesions of scurvy
•
Vitamin K deficiency, resulting in
hypoprothrombinemia, characterized by spontaneous bleeding and ecchymoses
•
Folic acid deficiency, resulting in macrocytic
anemia
The
threat of these avitaminoses provides the rationale for supplementing the diet
of every patient with chronic liver disease (especially if alcohol-related)
with ample quantities of vitamins A, B complex, C, and K and folic acid.
Metabolic Abnormalities
Abnormalities
of glucose metabolism also occur; the blood glu-cose level may be abnormally
high shortly after a meal (a diabetic-type glucose tolerance test result), but
hypoglycemia may occur during fasting because of decreased hepatic glycogen
reserves and decreased gluconeogenesis. Because the ability to metabo-lize
medications is decreased, medications must be used cau-tiously and usual
medication dosages must be reduced for the patient with liver failure.
Many
endocrine abnormalities also occur with liver dys-function because the liver
cannot metabolize hormones nor-mally, including androgens or sex hormones.
Gynecomastia, amenorrhea, testicular atrophy, loss of pubic hair in the male,
and menstrual irregularities in the female and other distur-bances of sexual
function and sex characteristics are thought to result from failure of the
damaged liver to inactivate estrogens normally.
Pruritus and Other Skin Changes
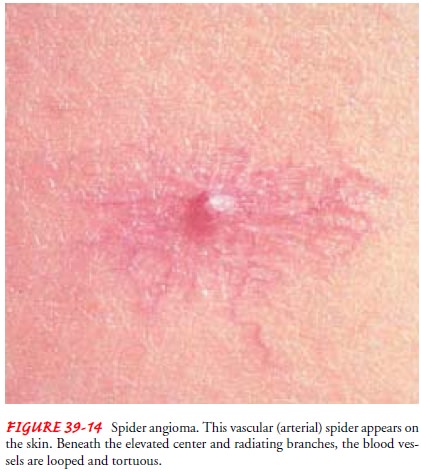
Patients
with liver dysfunction resulting from biliary obstruction commonly develop
severe itching (pruritus) due to retention of bile salts. Patients may develop
vascular (or arterial) spider angiomas (Fig. 39-14) on the skin, generally
above the waistline. These are numerous small vessels resembling a spider’s
legs. These are most frequently associated with cirrhosis, especially in
alcoholic liver dis-ease. Patients may also develop reddened palms (“liver
palms” or palmar erythema).
Related Topics