Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Diabetes Mellitus
Nursing Process: The Patient Newly Diagnosed With Diabetes Mellitus
NURSING PROCESS: THE PATIENT
NEWLY DIAGNOSED WITH DIABETES MELLITUS
Assessment
The
history and physical assessment focus on the signs and symp-toms of prolonged
hyperglycemia and on physical, social, and emotional factors that may affect
the patient’s ability to learn and perform diabetes self-care activities. The
patient is asked to de-scribe symptoms that preceded the diagnosis of diabetes,
such as polyuria, polydipsia, polyphagia, skin dryness, blurred vision, weight
loss, vaginal itching, and nonhealing ulcers. The blood glucose and, for
patients with type 1 diabetes, urine ketone levels are measured.
Patients
with type 1 diabetes are assessed for signs of DKA, in-cluding ketonuria,
Kussmaul respirations, orthostatic hypoten-sion, and lethargy. The patient is
questioned about symptoms of DKA, such as nausea, vomiting, and abdominal pain.
Laboratory values are monitored for metabolic acidosis (ie, decreased pH and
decreased bicarbonate level) and for electrolyte imbalance. Patients with type
2 diabetes are assessed for signs of HHNS, in-cluding hypotension, altered
sensorium, seizures, and decreased skin turgor. Laboratory values are monitored
for hyperosmolality and electrolyte imbalance.
If the
patient exhibits signs and symptoms of DKA or HHNS, nursing care first focuses
on treatment of these acute complica-tions, as outlined in previous sections.
Once these complications are resolving, nursing care then focuses on long-term
manage-ment of diabetes, as discussed in this section.
Then
the patient is assessed for physical factors that may im-pair his or her
ability to learn or perform self-care skills, such as:
•
Visual deficits (the patient is asked to read
numbers or words on the insulin syringe, menu, newspaper, or written teaching
materials)
•
Deficits in motor coordination (the patient is
observed eating or performing other tasks or handling a syringe or
finger-lancing device)
•
Neurologic deficits (eg, due to stroke, other
neurologic dis-orders; other disabling conditions) (from history in chart; the
patient is assessed for aphasia or decreased ability to fol-low simple
commands)
The
nurse evaluates the patient’s social situation for factors that may influence
the diabetes treatment and education plan, such as:
•
Low literacy level (may be evaluated while
assessing for visual deficits by having the patient read from teaching
materials)
•
Limited financial resources or lack of health
insurance
•
Presence or absence of family support
•
Typical daily schedule (patient is asked about
timing and number of usual daily meals, work and exercise schedule, plans for
travel)
The
patient’s emotional status is assessed by observing general demeanor (eg,
withdrawn, anxious) and body language (eg, avoids eye contact). The patient is
asked about major concerns and fears about diabetes; this allows the nurse to
assess for any mis-conceptions or misinformation regarding diabetes. Coping
skills are assessed by asking how the patient has dealt with difficult
situations in the past.
Diagnosis
NURSING DIAGNOSES
Based
on the assessment data, the patient’s major nursing diag-noses may include the
following:
•
Risk for fluid volume deficit related to polyuria
and dehy-dration
•
Imbalanced nutrition related to imbalance of
insulin, food, and physical activity
•
Deficient knowledge about diabetes self-care
skills/infor-mation
•
Potential self-care deficit related to physical
impairments or social factors
•
Anxiety related to loss of control, fear of
inability to man-age diabetes, misinformation related to diabetes, fear of
di-abetes complications
COLLABORATIVE PROBLEMS/ POTENTIAL COMPLICATIONS
Based
on assessment data, potential complications may include:
•
Fluid overload, pulmonary edema, heart failure
•
Hypokalemia
•
Hyperglycemia and ketoacidosis
•
Hypoglycemia
•
Cerebral edema
Planning and Goals
The
major goals for the patient may include maintenance of fluid and electrolyte
balance, optimal control of blood glucose levels, reversal of weight loss,
ability to perform survival diabetes skills and self-care activities, decreased
anxiety, and absence of complications.
Nursing Interventions
MAINTAINING FLUID AND ELECTROLYTE BALANCE
Intake
and output are measured. IV fluids and electrolytes are administered as
prescribed, and oral fluid intake is encouraged when it is permitted. Laboratory
values of serum electrolytes (especially sodium and potassium) are monitored.
Vital signs are monitored for signs of dehydration (tachycardia, orthostatic
hypotension).
IMPROVING NUTRITIONAL INTAKE
The
diet is planned with the control of glucose as the primary goal. It must take
into consideration the patient’s lifestyle, cul-tural background, activity
level, and food preferences. An appro-priate caloric intake allows the patient
to achieve and maintain the desired body weight. The patient is encouraged to
eat full meals and snacks as prescribed per the diabetic diet. Arrange-ments
are made with the dietitian for extra snacks before in-creased physical
activity. It is important for the nurse to ensure that insulin orders are
altered as needed for delays in eating be-cause of diagnostic and other
procedures.
REDUCING ANXIETY
The
nurse provides emotional support and sets aside time to talk with the patient
who wishes to express feelings, cry, or ask ques-tions about this new
diagnosis. Any misconceptions the patient or family may have regarding diabetes
are dispelled (see Table 41-7). The patient and family are assisted to focus on
learning self-care behaviors. The patient is encouraged to perform the skills
that are feared most and must be reassured that once a skill such as
self-injection or lancing a finger for glucose monitoring is performed for the
first time, anxiety will decrease. Positive reinforcement is given for the
self-care behaviors attempted, even if the technique is not yet completely mastered.
IMPROVING SELF-CARE
Patient
teaching is the major strategy used to prepare the pa-tient for self-care.
Special equipment may be needed for instruc-tion on diabetes survival skills,
such as a magnifying glass for insulin preparation or an injection-aid device
for insulin injec-tion. Low-literacy information and literature in other
languages can be obtained from the ADA. The family is also taught so that they
can assist in diabetes management by, for instance, prefill-ing syringes or
monitoring the blood glucose level. The diabetes specialist is consulted
regarding various blood glucose monitors and other equipment for use by
patients with physical impair-ments. The patient is assisted in identifying
community resources for education and supplies as needed. Other members of the
health care team are informed about variations in the timing of meals and the
work schedule (eg, if the patient works at night or in the evenings and sleeps
during the day) so that the diabetes treatment regimen can be adjusted accordingly.
MONITORING AND MANAGING POTENTIAL COMPLICATIONS
Fluid Overload
Fluid
overload can occur because of the administration of a large volume of fluid at
a rapid rate that is often required to treat the patient with DKA or HHNS. This
risk is increased in elderly pa-tients and in those with preexisting cardiac
disease. To avoid fluid overload and resulting congestive heart failure and
pul-monary edema, the nurse monitors the patient closely during treatment by
measuring vital signs at frequent intervals. Central venous pressure monitoring
and hemodynamic monitoring may be initiated to provide additional measures of
the fluid status. Physical examination focuses on assessment of cardiac rate
and rhythm, breath sounds, venous distention, skin turgor, and urine output.
The nurse monitors fluid intake and keeps careful records of IV and other fluid
intake, along with urine output measurements.
Hypokalemia
As
previously described, hypokalemia is a potential complication during the
treatment of DKA as potassium is lost from body stores. Low serum potassium
levels may result from rehydration, increased urinary excretion of potassium,
and movement of potassium from the extracellular fluid into the cells with
insulin administration. Prevention of hypokalemia includes cautious
re-placement of potassium; before its administration, however, it is important
to ensure that the patient’s kidneys are functioning. Because of the adverse
effects of hypokalemia on cardiac function, monitoring of the cardiac rate,
cardiac rhythm, electrocardio-gram, and serum potassium levels is essential.
Hyperglycemia and Ketoacidosis
Although
the hyperglycemia and ketoacidosis that may have led to the new diagnosis of
diabetes may be resolved, the patient is at risk for their subsequent
recurrence. Therefore, blood glucose levels and urine ketones are monitored,
and medications (insulin, oral antidiabetic agents) are administered as
prescribed. The pa-tient is monitored for signs and symptoms of impending
hyper-glycemia and ketoacidosis; if they occur, insulin and IV fluids are
administered.
Hypoglycemia
Hypoglycemia
may occur if the patient skips or delays meals or does not follow the
prescribed diet or greatly increases the amount of exercise without modifying
diet and insulin. Also, the hospitalized patient or outpatient who fasts in
preparation for di-agnostic testing is at risk for hypoglycemia. Juice or
glucose tablets are used for treatment of hypoglycemia. The patient is
en-couraged to eat full meals and snacks as prescribed per the dia-betic diet.
If hypoglycemia is a recurrent problem, the total therapeutic regimen should be
re-evaluated.
Because
of the risk of hypoglycemia, especially with intensive insulin regimens, it is
important for the nurse to review with the patient its signs and symptoms,
possible causes, and measures to prevent and treat it. The nurse stresses to
the patient and family the importance of having information on diabetes at home
for reference.
Cerebral Edema
Although
the cause of cerebral edema is unknown, it is thought to be caused by rapid
correction of hyperglycemia, resulting in fluid shifts. Cerebral edema can be
prevented by gradual reduc-tion in the blood glucose level (ADA, Hyperglycemic
Crises in Patients With Diabetes Mellitus, 2003). An hourly flow sheet is used
to enable close monitoring of the blood glucose level, serum electrolyte
levels, urine output, mental status, and neurologic signs. Precautions are
taken to minimize activities that could in-crease intracranial pressure.
PROMOTING HOME AND COMMUNITY-BASED CARE
Teaching Patients Self-Care
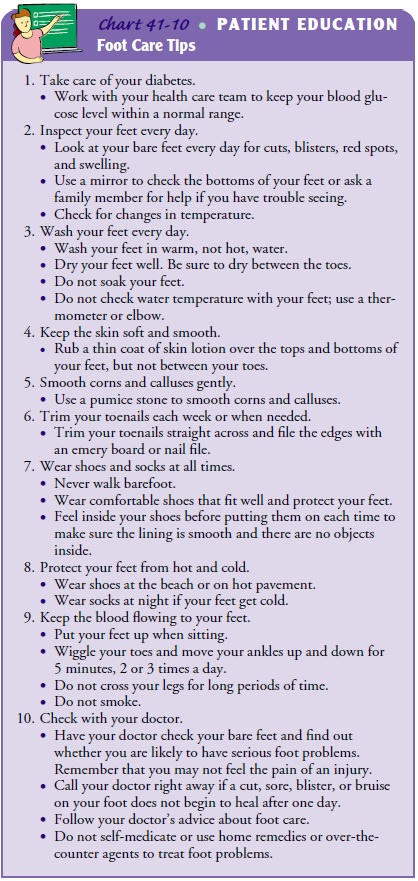
The
patient is taught survival skills, including simple pathophys-iology; treatment
modalities (insulin administration, monitoring of blood glucose, and, for type
1 diabetes, urine ketones, and diet); recognition, treatment, and prevention of
acute complica-tions (hypoglycemia and hyperglycemia); and practical
informa-tion (where to obtain supplies, when to call the physician). If the
patient has signs of long-term diabetes complications at the time of diagnosis
of diabetes, teaching about appropriate preventive behaviors (eg, foot care or
eye care) should be included at this time (Chart 41-10).
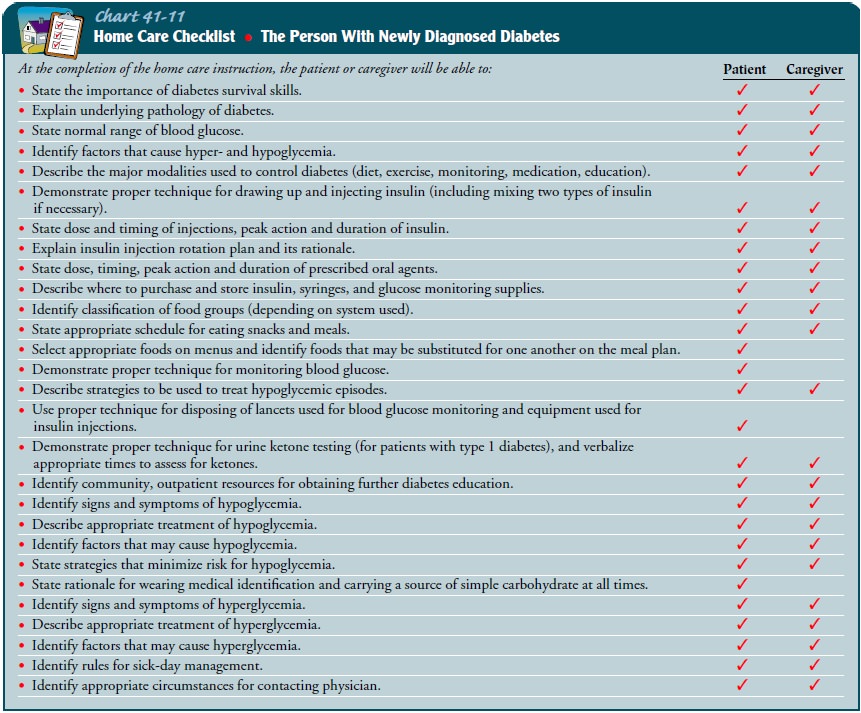
Continuing Care
Follow-up education is arranged with a home care nurse or an outpatient diabetes education center. This is particularly impor-tant for the patient who has had difficulty coping with the diag-nosis, the patient who has limitations that may affect his or her ability to learn or to carry out the management plan, or the patient without any family or social supports.
Referral to social services and community resources (eg,
centers for the visually impaired) may be needed, depending on the patient’s
financial circumstances and physical limitations. The importance of self-monitoring
and of monitoring and follow-up by primary health care providers is reinforced,
and the patient is reminded about the importance of keeping follow-up
appointments. The patient who is newly diagnosed with diabetes is also reminded
about the importance of participating in other health promotion activities and
health screening. Chart 41-11 is a checklist of home care skills.
Evaluation
EXPECTED PATIENT OUTCOMES
Expected
patient outcomes may include:
•
Achieves fluid and electrolyte balance
a)
Demonstrates intake and output balance
b)
Exhibits electrolyte values within normal limits
c)
Exhibits vital signs that remain stable with
resolution of orthostatic hypotension and tachycardia
•
Achieves metabolic balance
a)
Avoids extremes of glucose levels (hypoglycemia or
hy-perglycemia)
b)
Demonstrates rapid resolution of hypoglycemic
episodes
c)
Avoids further weight loss (if applicable) and
begins to approach desired weight
•
Demonstrates/verbalizes diabetes survival skills
a) Defines diabetes as a condition
in which high blood glu-cose levels are present
b) States normal and target
blood glucose ranges
c) Identifies factors that
cause the blood glucose level to fall (insulin, exercise, some oral
anti-diabetes medications)
d) Identifies factors that
cause the blood glucose level to rise (food, illness, stress, and infections)
e) Describes the major
treatment modalities: diet, exercise, monitoring, medication, education
f) Demonstrates proper
technique for drawing up and in-jecting insulin (including mixing two types of
insulin if necessary)
g) States dose and timing
of injections, peak action, dura-tion, and adverse effects of insulin
h) Verbalizes plan for
rotating insulin injection sites
i) States dose, timing,
peak action, and duration of pre-scribed oral agents
j) Verbalizes understanding
of food group classifications (depending on system used)
k) Verbalizes appropriate
schedule for eating snacks and meals; orders appropriate foods on menus;
identifies foods that may be substituted for one another on the meal plan
l) Demonstrates proper
technique for monitoring blood glucose, including using finger-lancing device;
obtain-ing a drop of blood; applying blood properly to strip; obtaining value
of blood glucose; and recording blood glucose value. Also, is able to calibrate
and clean meter, change batteries, identify alarms and warnings on meter, and
use control solutions to validate strips.
m) Demonstrates proper
technique for disposing of lancets and needles used for blood glucose
monitoring and in-sulin injections (discarding them into hard plastic
con-tainer such as empty bleach or detergent container or medical waste
containers)
n) Demonstrates proper
technique for urine ketone testing (for patients with type 1 diabetes) and
verbalizes appro-priate times to assess for ketones (when ill or when blood
glucose test results are repeatedly and inexplicably more than 250 to 300 mg/dL
[13.8 to 16.6 mmol/L])
o) Identifies community,
outpatient resources for obtain-ing further diabetes education
p) Identifies acute
complications (hypoglycemia and hyper-glycemia)
q) Verbalizes symptoms of
hypoglycemia (shakiness, sweat-ing, headache, hunger, numbness or tingling of
lips or fingers, weakness, fatigue, difficulty concentrating, change of mood)
and dangers of untreated hypo-glycemia (seizures and coma)
r) Identifies appropriate
treatment of hypoglycemia, in-cluding 15 g simple carbohydrate (eg, two to four
glu-cose tablets, 4 to 6 oz juice or soda, 2 to 3 teaspoons sugar, or 6 to 10
hard candies) followed by a snack of protein and carbohydrate (eg, cheese and
crackers or milk) or by a regularly scheduled meal
s) States potential causes
of hypoglycemia (too much in-sulin, delayed or decreased food intake, increased
phys-ical activity) and verbalizes preventive behaviors, such as frequent
monitoring of blood glucose when daily schedule is changed and eating a snack
before exercise
t) Verbalizes importance of
wearing medical identification and carrying a source of simple carbohydrate at
all times
u) Verbalizes symptoms of
prolonged hyperglycemia (in-creased thirst and urination)
v) Verbalizes rules for
sick day management
w) Describes where to
purchase and store insulin, syringes, and glucose monitoring supplies
x) Identifies appropriate
circumstances for calling the physi-cian (when ill, when glucose levels
repeatedly exceed a certain level [per physician guidelines], or when skin
wounds fail to heal) and also identifies name of physi-cian (or other health
care team member) and 24-hour phone number
•
Absence of complications
a)
Exhibits normal cardiac rate and rhythm and normal
breath sounds
b)
Exhibits jugular venous pressure and distention
within normal limits
c) Exhibits blood glucose
and urine ketone levels within normal limits
d)
Exhibits no manifestations of hypoglycemia or
hyper-glycemia
e)
Shows improved mental status without signs of cerebral
edema
f)
States measures to prevent complications
Related Topics