Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Diabetes Mellitus
Gestational Diabetes
GESTATIONAL
DIABETES
Gestational
diabetes is any degree of glucose intolerance with its onset during pregnancy.
Hyperglycemia develops during preg-nancy because of the secretion of placental
hormones, which causes insulin resistance. For women who meet one or more of
the fol-lowing criteria, selective screening for diabetes during pregnancy is
now being recommended between the 24th and 28th weeks of gestation: age 25
years or older; age 25 years or younger and obese; family history of diabetes
in first-degree relatives; or member of an ethnic/racial group with a high
prevalence of dia-betes (eg, Hispanic American, Native American, Asian
American, African American, or Pacific Islander).
Gestational
diabetes occurs in up to 14% of pregnant women and increases their risk for
hypertensive disorders during pregnancy (ADA, Gestational Diabetes Mellitus,
2003). Initial management includes dietary modification and blood glucose
monitoring. If hyperglycemia persists, insulin is prescribed. Oral antidiabetic
agents should not be used during pregnancy. Goals for blood glu-cose levels
during pregnancy are 105 mg/dL (5.8 mmol/L) or less before meals and 120 mg/dL
(6.7 mmol/L) or less 2 hours after meals (ADA, Gestational Diabetes Mellitus,
2003).
After
delivery of the infant, blood glucose levels in the woman with gestational
diabetes return to normal. However, many women who have had gestational
diabetes develop type 2 diabetes later in life. Therefore, all women who have
had gestational diabetes should be counseled to maintain their ideal body
weight and to exercise regularly to reduce their risk for type 2 diabetes (ADA,
Gestational Diabetes Mellitus, 2003).
CLINICAL MANIFESTATIONS
Clinical
manifestations of all types of diabetes include the “three Ps”: polyuria,
polydipsia, and polyphagia. Polyuria (increased uri-nation) and polydipsia
(increased thirst) occur as a result of the excess loss of fluid associated
with osmotic diuresis. The patient also experiences polyphagia (increased
appetite) resulting from the catabolic state induced by insulin deficiency and
the break-down of proteins and fats. Other symptoms include fatigue and
weakness, sudden vision changes, tingling or numbness in hands or feet, dry
skin, skin lesions or wounds that are slow to heal, and recurrent infections.
The onset of type 1 diabetes may also be as-sociated with sudden weight loss or
nausea, vomiting, or abdom-inal pains, if DKA has developed.
ASSESSMENT AND DIAGNOSTIC FINDINGS
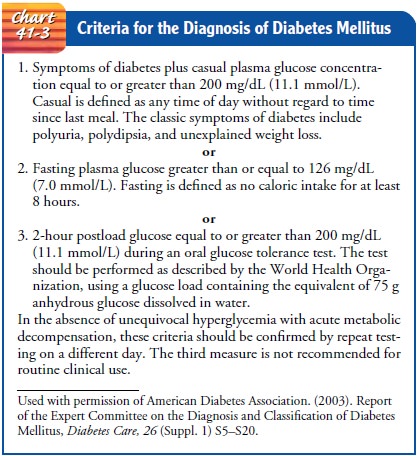
An
abnormally high blood glucose level is the basic criterion for the diabetes
diagnosis. Fasting plasma glucose
(FPG) levels of 126 mg/dL (7.0 mmol/L) or more or random plasma glucose levels
exceeding 200 mg/dL (11.1 mmol/L) on more than one occasion are diagnostic of
diabetes. The oral glucose tolerance test and the intravenous glucose tolerance
test are no longer recom-mended for routine clinical use. See Chart 41-3 for
the ADA’s di-agnostic criteria for diabetes mellitus (ADA, Expert Committee on
the Diagnosis and Classification of Diabetes Mellitus, 2003).
Plasma
glucose values may be 10% to 15% higher than whole blood values, which are
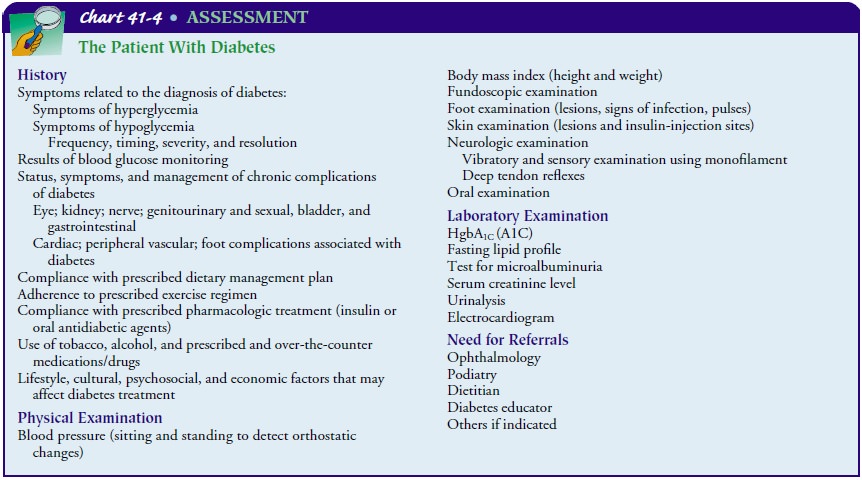
obtained with finger sticks (Porth, 2002). In addition to the assessment and
diagnostic evaluation per-formed to diagnose diabetes, ongoing specialized
assessment of patients with known diabetes and evaluation for complications in
patients with newly diagnosed diabetes are important compo-nents of care.
Parameters that should be regularly assessed are dis-cussed in Chart 41-4.
Gerontologic Considerations
Elevated
blood glucose levels appear to be age-related and occur in both men and women
throughout the world. Elevated blood glucose levels commonly appear in the
fifth decade of life and increase in frequency with advancing age. When elderly
people with overt diabetes are excluded from the statistics, approximately 10%
to 30% of elderly people have age-related hyperglycemia. What causes
age-related changes in carbohydrate metabolism is unresolved. Possibilities
include poor diet, physical inactivity, a decrease in the lean body mass in
which ingested carbohydrate may be stored, altered insulin secretion, and increase
in fat tissue, which increases insulin resistance.
Related Topics