Chapter: Medical Surgical Nursing: Assessment and Management of Patients With Eye and Vision Disorders
Dry Eye Syndrome
Infectious and Inflammatory
Conditions
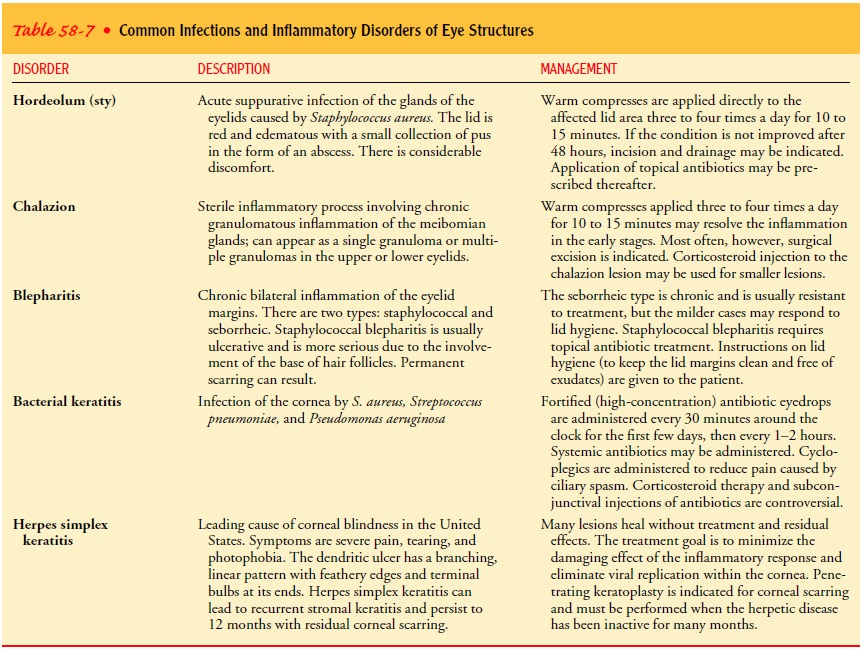
Inflammation
and infection of eye structures are common. Eye infection is a leading cause of
blindness worldwide. Table 58-7 describes selected common infections and their
treatment.
DRY EYE SYNDROME
Dry eye syndrome, or keratoconjunctivitis sicca, is
a deficiency in the production of any of the aqueous, mucin, or lipid tear film
components; lid surface abnormalities; or epithelial abnormali-ties related to
systemic diseases (eg, thyroid disorders, Parkinson’s disease), infection,
injury, or complications of medications (eg, antihistamines, oral
contraceptives, phenothiazines).
Clinical Manifestations
The most common complaint in dry eye syndrome is a
scratchy or foreign body sensation. Other symptoms include itching, ex-cessive
mucus secretion, inability to produce tears, a burning sen-sation, redness,
pain, and difficulty moving the lids.
Assessment and Diagnostic Findings
Slit-lamp examination shows an absent or
interrupted tear menis-cus at the lower lid margin, and the conjunctiva is
thickened, ede-matous, hyperemic, and has lost its luster. A tear meniscus is
the crescent-shaped edge of the tear film in the lower lid margin. Chronic dry
eyes may result in chronic conjunctival and corneal irritation that can lead to
corneal erosion, scarring, ulceration, thinning, or perforation that can
seriously threaten vision. Sec-ondary bacterial infection can occur.
Management
Management
of dry eye syndrome requires the complete cooper-ation of the patient with a
regimen that needs to be followed at home for a long period, or complete relief
of symptoms is un-likely. Instillation of artificial tears during the day and
an oint-ment at night is the usual regimen to hydrate and lubricate the eye
through stimulating tears and preserving a moist ocular sur-face.
Anti-inflammatory medications are also used, and moisture chambers (eg,
moisture chamber spectacles, swim goggles) may provide additional relief.
Patients may become hypersensitive to chemical
preservatives such as benzalkonium chloride and thimerosal. For these
pa-tients, preservative-free ophthalmic solutions are used. Manage-ment of the
dry eye syndrome also includes the concurrent treatment of infections, such as
chronic blepharitis and acne rosacea, and treating the underlying systemic
disease, such as Sjögren’s syndrome (an autoimmune disease).
In advanced cases of dry eye syndrome, surgical treatment that includes punctal occlusion, grafting procedures, and lateral tar-sorrhaphy (ie, uniting the edges of the lids) are options. Punctal plugs are made of silicone material for the temporary or perma-nent occlusion of the puncta. This helps preserve the natural tears and prolongs the effects of artificial tears. Short-term occlusion is performed by inserting punctal or silicone rods in all four puncta. If tearing is induced, the upper plugs are removed, and the re-maining lower plugs are removed in another week. Permanent occlusion is performed only in severe cases among adults who do not develop tearing after partial occlusion and who have results on a repeated Schirmer’s test of 2 mm or less (filter paper is used to measure tear production).
Related Topics